Title: Mullen, F.
Source text: The Medical and Surgical History of the War of the Rebellion. (1861-65.), Part 3, Volume 2 (Washington, DC: Government Printing Office, 1883), 539.
Civil War Washington ID: med.d2e20758
TEI/XML: med.d2e20758.xml
CASE 787.—Private F. Mullen, Co. E, 43d New York, aged 21 years, was wounded in the left leg, at Fredericksburg, May 3, 1863, and subsequently underwent secondary amputation. Surgeon J. A. Lidell, U. S. V., who performed the operation,¹ forwarded the following descriptive history: "The wound was caused by a minié ball, which passed through and fractured the tibia in the lower third. The man was brought to Stanton Hospital, Washington, three days afterwards. His general condition was good, and it was judged expedient to attempt to save the limb without operation. It was accordingly placed in Hodgen's splint and cold-water dressings were applied; stimulants administered. After several days the parts suppurated freely, and by June 1st the wounds were discharging a good and healthy pus, consolidation taking place, and appetite and pulse being normal. The parts continued to heal nicely up to July 28th, when the patient fell and re-fractured the limb while attempting to walk across the Ward. On August 2d, several pieces of bone were removed. August 15th, parts œdematous; discharge thin and fetid. On August 19th, several openings for the exit of pus were made, when a small necrosed splinter came away; pulse weak; general health suffering. The leg remained in about the same condition until September 1st, when compression by bandage was applied. About October 1st there was both general and local improvement, the discharge being of a thick and healthier character. The splints were now removed and stimulants continued. One month later necrosis of the shaft of the tibia had become extensive, the dead bone being completely encased in an involucrum; condition fair; discharges from several openings. But little change took place up to December 1st, and none for the better for one month afterwards. The involucrum was now large and the skin covering the front of it thin and about to ulcerate extensively; the foot being considerably twisted inward by abnormal muscular action (partial talipes varus) and the deformity steadily increasing; ankle joint also becoming stiff. There being now no hopes of preserving a useful limb it was deemed advisable to remove it by amputation. The operation was performed on January 9th, at the junction of the upper and middle thirds, by the flap method (double flaps, the anterior one being short). The sawn end of the tibia was beveled off as recommended by Sanson, that is, by placing the saw obliquely—not on the ridge, but on the internal surface of the bone. The fibula was divided somewhat higher up than the tibia, as practised by Roux. Throughout the operation the patient was kept insensible by sulphuric ether. He did not exhibit any perceptible shock. The flaps were carefully coaptated and secured at several points by interrupted sutures and strips of isinglass plaster. Several turns of a roller were placed around the leg to serve as a supporting bandage; but no other dressing was applied. A full anodyne was administered after the operation and another at 12 P. M. On the following day the patient was sitting up in bed reading a newspaper, the stump being in fine condition, free from heat and redness, and almost devoid of pain and swelling. On January 13th the sutures were removed and the stump was dressed for the first time and found to be uniting by primary adhesion. There was no constitutional disturbance whatever. On January 24th the last ligature, that of the posterior tibial artery, came away. The patient had not at any time nor in any way suffered in consequence of the amputation, and the stump had united by first intention. In short, he recovered precisely in the same way as the most fortunate cases of amputation of the leg on account of disease get well." The amputated bones of the leg (Spec. 2022) were contributed to the Museum by the operator and are represented in the wood-cut (FIG. 313), showing the fractured tibia, with an abundant involucrum formed to nearly the point of section, and a large detached but imprisoned sequestrum being exhibited through the cloacæ. A few points of osseous deposit are also seen on the fibula, which is uninjured. The patient entirely recovered, and was ultimately discharged September 5, 1864, and pensioned. In his application for commutation, dated 1870, he described the condition of the stump as being "in good order." He died March 5, 1871. The cause of his death has not been ascertained.
¹ LlDELL (J. A.), On the Major Amputations for Injuries in both Civil and Military Practice, in Am. Jour. Med. Sciences, 1864, Vol. XLVII, p. 376.
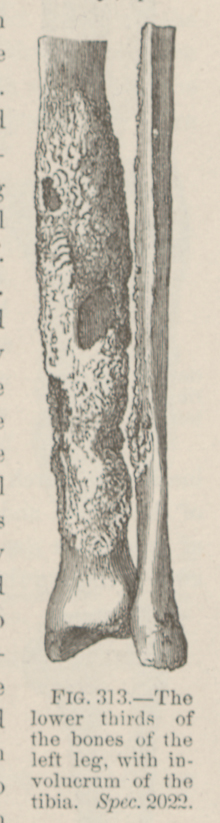 FIG. 313.—The lower thirds of the bones of the left leg,
with involucrum of the tibia. Spec. 2022.
FIG. 313.—The lower thirds of the bones of the left leg,
with involucrum of the tibia. Spec. 2022.