Title: Barnett, D. A.
Source text: The Medical and Surgical History of the War of the Rebellion. (1861-65.), Part 3, Volume 2 (Washington, DC: Government Printing Office, 1883), 292-293.
Civil War Washington ID: med.d2e13119
TEI/XML: med.d2e13119.xml
CASE 472.—Sergeant D. A. Barnett, Co. B, 99th Pennsylvania, aged 22 years, was wounded at Kelly's Ford, November 7, 1863. Surgeon J. W. Lyman, U. S. V., recorded his admission to the field hospital of the 1st division, Third Corps, with "shot wound of left knee joint." Two days after the reception of the injury the wounded man was transferred to Douglas Hospital, Washington, whence Assistant Surgeon W. Thomson, U. S. A., reported the following history: "The patient was anæmic when admitted, and stated that very free hæmorrhage took place the moment he was wounded. He was struck by a bullet, which entered the leg at the lower border of the patella, and was removed through an incision at the median line posteriorly, four inches above the joint. An examination showed the probable obliteration of the main vessel, since there was no circulation in the foot, which, with the leg half way to the knee, was cold and purple or tallow colored, and in the early stages of traumatic sphacelus. This, added to the direct wound of the knee joint, rendered an operation necessary, which was performed on November 10th. Ether was given, and the limb was removed by Acting Assistant Surgeon P. R. Holly, at the lower third of the thigh, by the circular method, with a straight cut from the wound of exit to the point of the circular incision. The operation was well borne and there was no serious loss of blood. On examining the amputated leg, I found that the ball had comminuted the patella and passed through the femur, entering at the outer margin of the inner condyle and dividing the popliteal artery. The popliteal space contained a large quantity of coagulated blood, and the ends of the vessel were surrounded by a mass of pink-colored and semi-organized clot, sufficiently firm to prevent hæmorrhage. The patient's tongue was very pallid and his whole appearance anæmic. His leg soon became swollen though perfectly white, resembling a case of phlegmasia alba dolens. The skin was smooth and blanched; there was tenderness along the line of the bone and no vigorous effort at repair, the edges of the incision being pale. The discharge consisted of dark colored ill-looking pus, and the whole appearance of the stump was unfavorable; the edges gaped widely apart. On November 20th, a slight slough appeared on the posterior lip of the stump, and two days afterwards the patient had a severe chill, followed by profuse perspiration in the night and succeeded by a light cough. During the night of the 23d there was another severe chill, and the next day respiration was increased in frequency and accompanied by pain in the right side. There was no perceptible dullness on percussion, but on auscultation it was found that inspiration was deep and a little labored, while the expiration over both lungs anteriorly was prolonged almost as in phthisis. There was no rale, but the expiratory sound seemed to indicate that the whole lung had lost some of its elasticity and returned upon itself after dilatation with apparent difficulty. Expectoration was slight, very tough and viscid; the pulse rapid and feeble; the skin relaxed. The pulse became still weaker, and the respiration more hurried until almost sighing; the nervous depression increased. The breath had the sweet sickening smell resembling the odor of fermentation, which denotes pyæmia. Death occurred at 8 A. M. on November 26, 1863. The post-mortem examination was made six hours afterwards. On opening the right pleural cavity we found the lung coated with soft greenish colored lymph, and there was an effusion amounting to six ounces of yellow pus and serum, separating into two strata, the upper serum, the lower pus, and having (under the microscope) the usual pus corpuscles floating in a fluid with an abundance of unrecognizable debris. There seemed to be also a thin layer of pus beneath the pleura anteriorly, giving that portion of the lung a yellowish color. The upper lobe was apparently normal; the lower lobe posteriorly was congested, dark in color, and, on division, revealed nodules of tissue of various sizes in all stages of pathological changes from acute congestion to thorough hepatization and yellow softening. The diseased spots were in dimension from the size of half an English walnut to that of a split pea, the large ones having in the center a space white or yellow in color, and probably breaking down rapidly. The outline of these solidified portions, on section, suggested the idea of embolism, since they were somewhat triangular in shape, with the base at the pleural surface and the apex at the deepest portion of the lung, giving the impression that a circumscribed area of lung nourished by a single vessel had been destroyed by its occlusion. There was no recent effusion in the left pleural cavity, but changes in the parenchyma similar to those on the right side were discovered. An examination of the vessels of the stump revealed the existence of inflammation of the artery and veins. Both the femoral artery and vein at the point of their escape from the pelvis were normal. The femoral vein at the entrance of the saphena was filled with a semi-organized clot, which extended through the saphena and femoral to a point two inches from the cut ends of these vessels, where they had been divided on the face of the stump. (See left-hand figure of PLATE XX, opposite p. 294.) These vessels, as will be seen, are now hard and firm dark-red cords, of course entirely impervious. The artery from the origin of the profunda to a point two inches from its cut termination was also reddened, and its inner coat softened and easily removable. The phlebitis, with its occlusion of the main venous trunks, accounted for the swollen and white condition of the stump, compared above to the condition known as phlegmasia alba dolens. In making this dissection it was observed that the inflammation, apparent in the artery and to some extent circumscribed (since its lower extremity yet contained the clot formed on the application of the ligature and was normal both in color and firmness, as well as that which occluded the veins), had extended through the coats of these vessels from without. No pus was found in the veins, and no evidence of inflammation except the marked redness of the coats and the firm and clotted coagulation of the blood within." Wet preparations of the femoral and profunda arteries (Spec. 2246), the femoral and saphena veins (Spec. 3991), and the popliteal artery and vein (Spec. 2247), saved from the stump, were contributed to the Museum by Assistant Surgeon Thomson. Drawings of the specimens 3991 and 2246 were prepared by Hospital Steward Stauch, and are represented, the former on the left and the latter on the right side of PLATE XX, opposite p. 294.
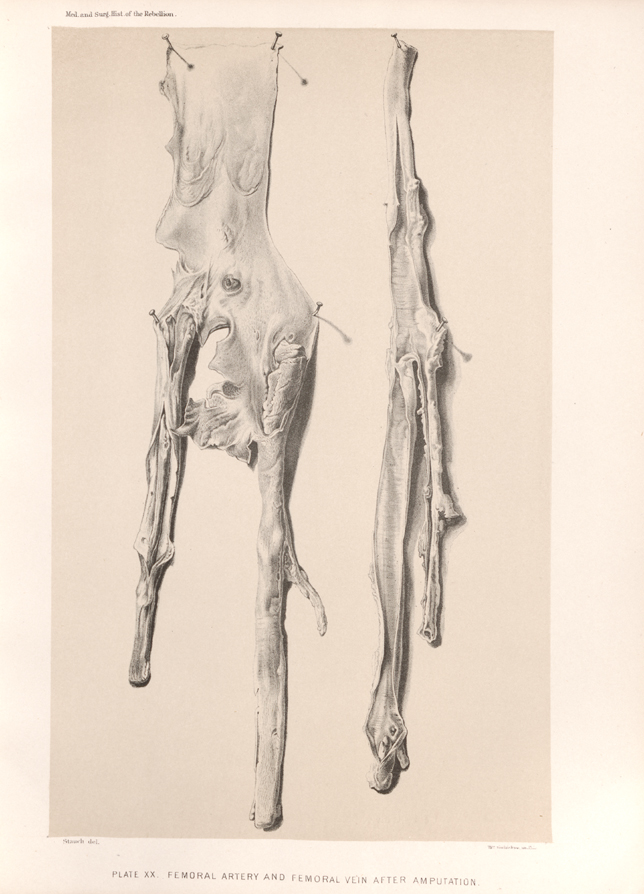 PLATE XX. FEMORAL ARTERY AND FEMORAL VEIN AFTER AMPUTATION.
PLATE XX. FEMORAL ARTERY AND FEMORAL VEIN AFTER AMPUTATION.