Title: Saxon, J. N.
Source text: The Medical and Surgical History of the War of the Rebellion. (1861-65.), Part 3, Volume 2 (Washington, DC: Government Printing Office, 1883), 290-291.
Civil War Washington ID: med.d2e12872
TEI/XML: med.d2e12872.xml
CASE 470.—Private J. N. Saxon,¹ Co. D, 9th Louisiana, aged 27 years, was wounded in the right knee, at Rappahannock Station, November 7, 1863, and suffered amputation at the Stanton Hospital, Washington. Surgeon J. A. Lidell, U. S. V., who performed the operation, described the case as follows: "A conical bullet entered the knee about three inches above the patella, on a line with its inner margin, passed backward, downward, and a little inward, and escaped at the inner posterior side, about six inches below the joint. The inner condyle of the femur was fractured by the missile passing through it, but without opening the cavity of the joint. The patient stated that his knee was bent at the time of the infliction of the wound. He was admitted two days after the injury and did well, having good spirits, good appetite, and but little pain or swelling of the parts until the night of November 16th, when he had a severe chill, accompanied with great pain in and about the knee, and the injured parts became hot and swollen. On the following morning he exhibited great constitutional disturbances: skin hot; tongue coated white; pulse very rapid, gaseous, and weak. The injured knee was much swollen and exquisitely tender, and he complained of intense pain in it; the anterior orifice of the wound presented a gelatinous appearance, with elevated and everted edges. The patient appeared so feeble that I thought he would not then bear the shock of an amputation, and ordered him to take whiskey freely with anodynes. The next day, November 18th, his general condition appeared unchanged with the exception of his pulse, which was stronger and not gaseous, being 120 by the watch. He had not slept during the night, and complained of great pain in the knee, which was rather more swelled, and the tumefaction was extending up the thigh. The wound presented the same gelatinous appearance as the day before, and the skin over the saphenous veins looked purple colored, but the veins did not exhibit any induration. The thigh was amputated at the lower third, by the flap method, at 1 P. M., about thirty-six hours subsequent to the accession of the secondary arthritis. The patient was under sulphuric ether and bore the operation well. Examination of the amputated member showed the inner condyle of the femur to be extensively comminuted. There was a layer of yellowish gray colored plastic exudation on the articulating surfaces of the fragments in the joint, and the cavity of the joint contained about three ounces of reddish brown colored liquid, in which shining globules floated resembling oil in appearance. The synovial membrane was reddened, especially the pouches of it in relation with the quadriceps extensor cruris. The subcutaneous areolar tissue was infiltrated with a yellowish serum. The bullet was ascertained to have passed behind the joint. On the day following the operation the patient's tongue was coated and his appetite poor; he had also moderate diarrhœa, the evacuations being very offensive. Five grains of blue mass was given at night, and free stimulation with whiskey. On the 20th, the patient was comfortable and the stump looked well. The diarrhœa was unchanged, but during the following several days it gradually abated and the patient progressed well in every respect. 28th, patient cheerful; tongue clean; appetite good; bowels regular; stump but little swollen; granulations healthy; suppuration moderate in quantity and laudable in quality. 30th, patient appeared to be doing well, but complained a good deal of pain in and about the stump. December 1st, patient restless and complaining of increased pain in the stump, especially about the end of the bone; no preternatural swelling, redness or heat in the stump. Prescribed one-fourth of a grain of sulphate of morphia and one drachm of Hoffman's anodyne every four hours. 2d, patient more restless, appearing much agitated and very nervous, having slept but little, and complaining of agonizing pain about end of bone and end of femoral artery. There were exacerbations in the pain and sometimes the whole stump ached, but there was no febrile excitement and nothing untoward in the appearance or feel of the stump; neither was it swelled, red, or hot. 3d, patient had a bad night, and complained much of sickening pain in end of stump and in bowels. About 7 A. M. the ligature separated and a most profuse hæmorrhage occurred, the blood pouring out in a stream as large as the calibre of the artery. It was finally stopped by digital compression, but, in the meantime, he had lost more than six pounds of blood, which brought him very low. He was stimulated as freely as possible with whiskey and carbonate of ammonia, but did not rally, and died about 3 P. M. Autopsy twenty-three hours after death: Surface of body very pale and waxy (exsanguinated); rigor mortis strong; superficial lymphatic ganglia lying along the vena saphena magna of amputated thigh all enlarged and exhibiting a faint reddish hue on section; deep ganglia not affected; stump not œdematous and no part sloughy; stump healed throughout except in the track of the ligatures and at the end of the bone. The femoral ligature had come away and the end of the vessel was patulous, uncontracted, and unobstructed. The coats of the artery were infiltrated with blood (recent) at its end and for about half an inch above it. A branch of considerable size was given off from the artery about three-fourths of an inch above its end, which had apparently interfered with the formation of a suitable clot for the permanent plugging up of the vessel; there had been but little effort towards occlusion. No other abnormity existed in the artery. The end of the femoral vein was well sealed up, the vein itself diminished in size up to the nearest valve, a distance of about an inch, and its walls thickened in same locality so as to equal those of the femoral artery; lining membrane not stained with blood; no emboli and no thrombi found anywhere, and no vein presenting any abnormity, the vena profunda not being overlooked. A remarkable osteophyte was found in relation with the femoral artery and vein at their respective ends in the stump. It was developed from (connected with) the linea aspera, a little above the end of the femur, and thence passed horizontally inward, separating or forking into distinct plates, toward the ends of which the one laid in front of and was closely adherent to that side of the artery at and near its end; the other laid behind and was adherent to the vein at and near its end. This osteophyte was about seven-eighths of an inch wide where broadest, and about one-fourth of an inch thick. It was of recent formation. The lower part of the femur in the stump was moderately enlarged by deposit (laminated) of new bone beneath the periosteum (hyper-nutrition); this membrane was detached for about one-fourth of an inch above the line of the saw all the way round the bone, which presented a dull white color in that locality. The medullary membrane was noticed to bulge out a good deal at the end of the bone and to present a dark red or reddish brown color. It was also strong and tough (flesh like). On sawing through the lower part of the femur lengthwise and cleaning off the bone dust the medullary membrane was seen to be more vascular than natural; the medullary tissue exhibited about a dozen small milk-colored abscesses on the surface of the section, showing pus under the microscope, and varying in size from that of a split pea to a mustard seed. The osseous tissue outside of the medullary canal was more compact and heavier than natural in the same locality. The periosteum was thickened to the extent of from one to three lines and more vascular than natural, the thickening being greatest where it had been detached from the bone. There was also a small abscess, flattened in shape, and holding about an ounce of cream-like pus, in the quadriceps extensor cruris muscle, and the red muscular tissue in immediate relation with it was changed to a dark brown color, which, however, did not extend to any depth. The spleen was enlarged, and the other organs all exsanguinated but presenting no other abnormity." The bones of the knee of the amputated limb (Spec. 1819), the femoral vein and artery (Spec. 1892), with portion of the osteophyte attached, and a longitudinal half section of the lower end of the stump of the femur (Spec. 1860, shown in FIG. 4 of PLATE XLIII, opposite p. 290) four and one-fourth inches long, were contributed to the Museum by the operator.
¹ LIDELL (J. A.), in Surgical Memoirs, * * by the United States Sanitary Commission, New York, 1870, Vol. I, p. 358, gives a detailed account of this case.
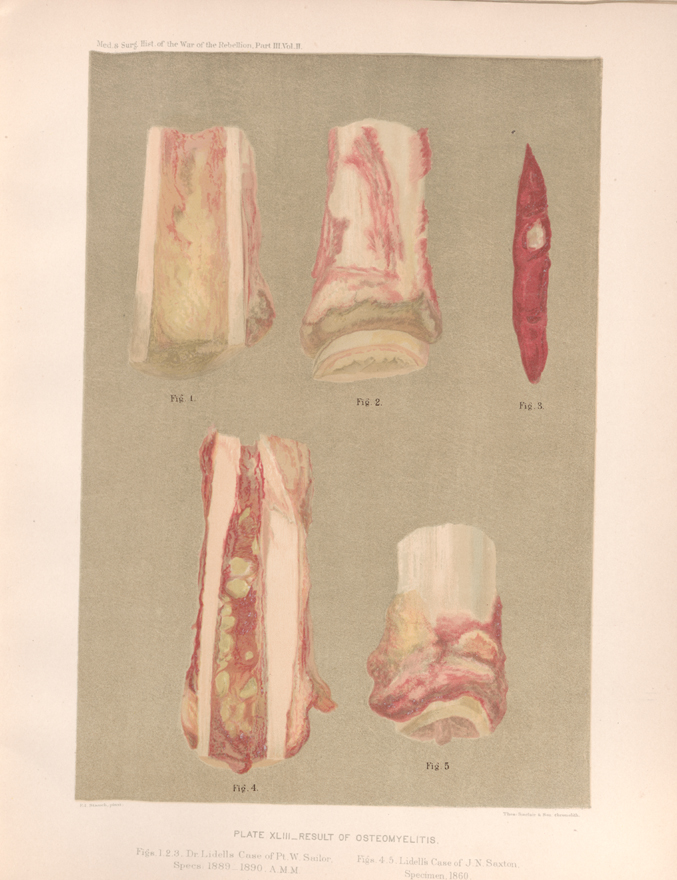 PLATE XLIII. __ RESULT OF OSTEOMYELITIS. Figs. 4, 5. Lidell's Case of J. N. Saxton, Specimen. 1860.
PLATE XLIII. __ RESULT OF OSTEOMYELITIS. Figs. 4, 5. Lidell's Case of J. N. Saxton, Specimen. 1860.