Title: Manchester, A. L.
Source text: The Medical and Surgical History of the War of the Rebellion. (1861-65.), Part 2, Volume 1 (Washington, DC: Government Printing Office, 1879), 519.
Civil War Washington ID: med.d1e41932
TEI/XML: med.d1e41932.xml
The extreme dimensions of the erosions, which occasionally result from the extension of follicular ulcers, are well illustrated by the plate facing page 526, which is a reproduction of a photograph of No. 195, Medical Section. The following is an account of the case:
CASE 904.—Sergeant A. L. Manchester, company E, 152d New York volunteers; age 23; was enlisted September 27, 1862, and continued to do duty with his company until March, 1863. During much of this time he had diarrhœa, which, however, did not prevent him from remaining on duty. March 2d, being then on duty as one of the guard at Douglas hospital, Washington, D. C., he was attacked by measles, with dry skin, pulse 110, and dark tongue. At the time of this attack he was a good deal broken down by the disorder of his bowels, and when, on the 5th of March, he was transferred to a bed in the hospital, the entry in the register was "measles and enteritis." The stools had been comparatively painless, but, March 7th, tormina and tenesmus supervened and they became bloody; they did not, however, exceed ten in twelve hours. These symptoms gradually abated under the use of a chalk mixture with opiate suppositories, and by the 12th of March the stools were reduced to four in the twenty-four hours, and were no longer bloody; skin moist; tongue cleaner; pulse 70, but quite feeble; the patient began to eat, and was now free from tenesmus and abdominal pain. March 20th: Is much better; pulse 84 and stronger; he sits up; has milk and eggs for diet; the remedies employed seem to control the tendency to pain and straining; the latter symptom appears to be kept in check by the use of the suppositories mentioned above. March 22d: Appetite better; only three painless passages in the last twenty-four hours; pulse 84; skin natural; tongue coated; slight tenderness on pressure in the left inguinal region. March 28th: Not so well; pulse 110; skin natural; has had about four stools daily for the last few days; they are dark-colored and stringy; tongue coated with a brownish fur; increased tenderness in left inguinal and lumbar regions. March 29th: Pulse 125; skin dry; tongue coated, but not so thickly as yesterday. Ordered quinia and milk punch. March 30th: Continual bilious vomiting set in, which was somewhat relieved by creasote, but it recurred from time to time, and death ensued April 1st. Stimulants, beef tea, &c., had been freely used during the last week of life. Autopsy: The small intestine near the ileocæcal valve was inflamed; higher up it was healthy. The large intestine was extensively inflamed and ulcerated.—Acting Assistant Surgeon Henry L. W. Burritt. [Nos. 194 and 195, Medical Section, Army Medical Museum, are from this case.]
The plate represents a portion of descending colon, which exhibits a number of the small, oval, characteristic follicular ulcers, but shows besides a number of large irregular ulcers with overhanging edges. The largest of these are more than an inch in diameter. It is probable that follicular ulceration had existed in this case for some time before the patient was attacked by measles, and that in consequence of the adynamic condition induced by that disease the ulcers rapidly extended. This seems to have been effected by a simple ulcerative process quite independent of any diphtheritic inflammation, and the specimens afford an excellent illustration of the great size to which catarrhal ulcers sometimes extend. No. 194, Medical Section, is taken from higher up the same colon, and exhibits similar lesions but in a less marked degree.
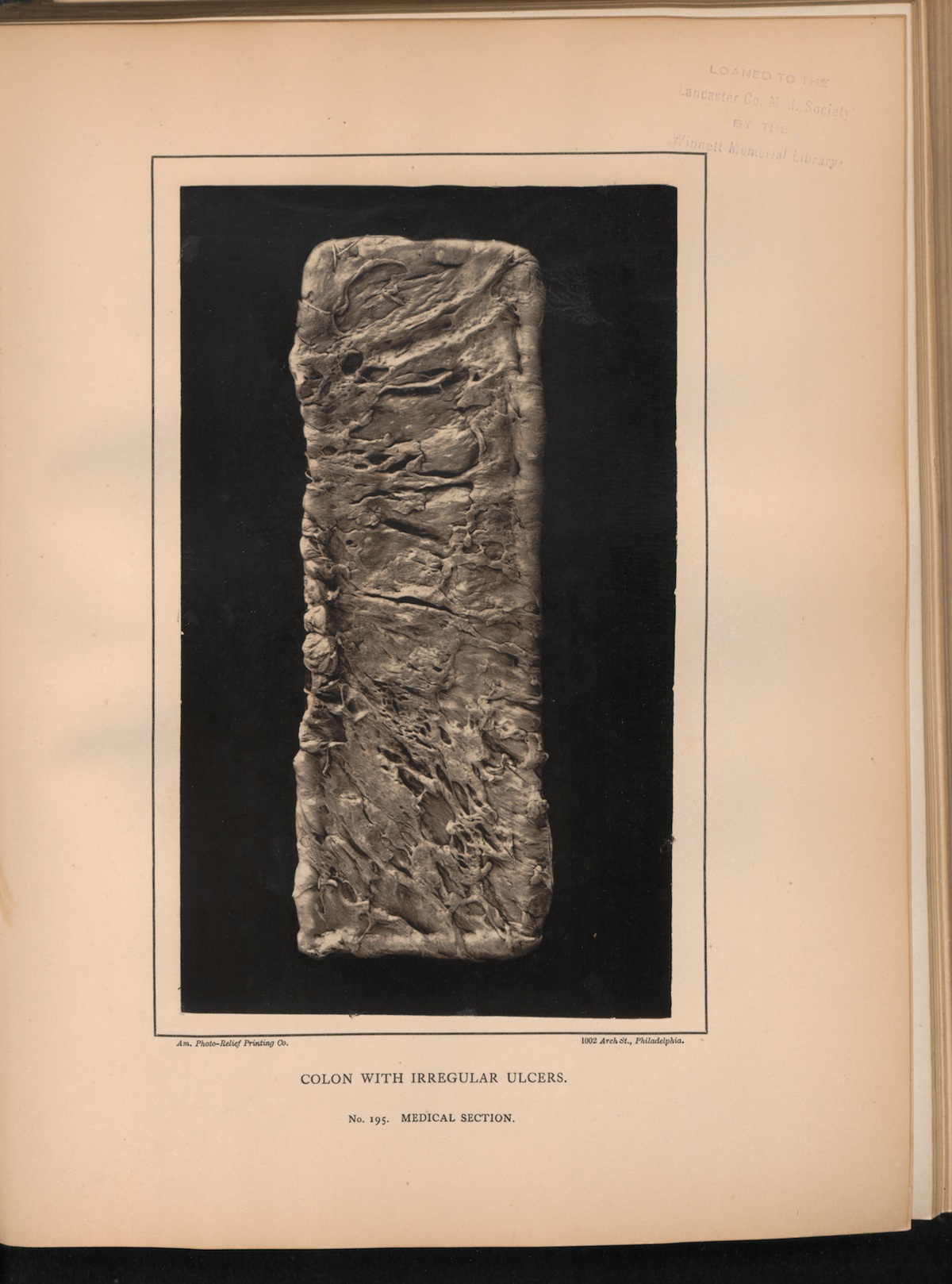 PLATE XXXIV. COLON WITH IRREGULAR ULCERS. No. 195. MEDICAL
SECTION.
PLATE XXXIV. COLON WITH IRREGULAR ULCERS. No. 195. MEDICAL
SECTION.