Title: Campbell, Ephraim
Source text: The Medical and Surgical History of the War of the Rebellion. (1861-65.), Part 2, Volume 1 (Washington, DC: Government Printing Office, 1879), 517-518.
Civil War Washington ID: med.d1e41929
TEI/XML: med.d1e41929.xml
The chromo plate facing page 520 represents follicular ulcers of the colon fringed with pseudomembrane. The following is an account of the case:
CASE 902.—Corporal Ephraim Campbell, company D, 150th Pennsylvania Volunteers; age 24; was admitted to the field hospital of the first division, fifth army corps, near Petersburg, Virginia, September 12, 1864. Diarrhœa: for which he had been treated in his regimental hospital. September 14th, he was transferred to the hospital of the 3d division, fifth corps, and September 29th, to the depot hospital of the fifth corps, at City Point, Virginia, where the diagnosis recorded was fever. Thence he was transferred to Columbian College hospital, Washington, D. C., where he was admitted, October 30th, suffering from all the symptoms of chronic diarrhœa. He was extremely emaciated, pulse 110 and small; had five or six loose dejections daily, and no appetite. Ordered hot fomentations to be applied to the abdomen, with rest in bed, and a diet of boiled milk and beef tea. November 2d, he reports that he feels better than on admission, and begins to relish his food a little, but the diarrhœa continues unabated. ℞. Chalk mixture three ounces, fluid extract of ginger half an ounce, tincture of cinchona one ounce; take a tablespoonful three times a day; continue the hot fomentations; extra diet. November 6th: Since the last note the patient has been better, but to-day is worse again. His bowels are moved every hour, and the dejections are mixed with blood; pulse 110 and thread like; abdomen tympanitic. His strength is less than yesterday; no appetite. Continue diet and treatment, with the addition of laudanum enemata. November 7th: The bowels are moved less frequently. The patient rested well last night, and has some appetite. Continue treatment. November 9th: Pulse 100; bowels again very loose, the dejections contain mucus and blood; appetite poor. Continue treatment. November 11th: The symptoms continue with little change, except that the patient complains of a dry cough at night; there is, however, no pain in the chest, and the respiration appears to be normal. Continue treatment, with the addition of a cough mixture containing syrup of senega and paregoric. November 14th: Pulse 96, skin dry and harsh, respiration 20 per minute, cough not so dry. The bowels were only moved twice since yesterday morning; appetite very poor. Continue treatment. November 15th: Pulse 108, respiration 32, bowels moved twelve times since yesterday morning; the dejections are bloody, strength failing, no appetite. ℞. Brandy four ounces, carbonate of ammonia two scruples; take a tablespoonful every three hours; beef tea. November 16th: Pulse 100, respiration 32, bowels very loose, strength failing fast. Continue treatment and diet. Died November 18th. Autopsy nine hours after death: Body very much emaciated. The right pleural cavity contained one gallon of sero-purulent fluid. The right lung was collapsed, coated with lymph and carnified. The left lung was normal. There was a large abscess in the upper portion of the liver which communicated with the pleural cavity through an opening in the diaphragm three by four inches in diameter. The fifth, sixth and seventh ribs were denuded of periosteum and bathed in pus. The omentum was quite devoid of fat. The mesenteric glands were enlarged. The spleen was normal. The mucous membrane of the lower portion of the ileum was coated with pseudomembrane and presented a number of small follicular ulcers. Peyer's patches were slightly thickened. The cæcum and colon were thickly studded with follicular ulcers, the edges of many of which were covered with pseudomembrane.—Acting Assistant Surgeon A. H. Wilson, U. S. A. [Nos. 433-437, Medical Section, Army Medical Museum, are from this case.]
The specimens from this case were brought to the Museum immediately after the autopsy, and a drawing in water colors representing a portion of the descending colon was made by Mr. Hermann Faber. The plate is a reproduction of this drawing. The mucous surface is seen to be generally reddened, with grayish streaks and patches. There are a considerable number of follicular ulcers, the smallest of which are rounded and very minute, while the larger ones, varying from ⅒th to ¼th of an inch in long diameter, are usually oval; the edges of most of these ulcers are fringed with curdy yellow pseudomembrane. The submucous tissue was considerably thickened, as is well shown on the left hand of the piece near the bottom where its edge comes into view. This specimen has been preserved in the Museum, No. 437, Medical Section. The other specimens from the same case are: No. 436, the appendix vermiformis and a part of the caecum, showing similar ulcers; No. 433, the collapsed right lung, thickly coated with pseudomembrane; No. 435, a portion of the liver, showing a large abscess cavity on its upper surface; and No. 434, the seventh rib, showing the effects of the burrowing of the pus from the abscess in its efforts to escape; the pulmonary surface of the bone is denuded of periosteum, and presents several flat new-formations of bony tissue. It would appear that in this case the large hepatic abscess entirely escaped observation during life, and the remark in the history of the case, on the 11th of November, only a week before death, that "the respiration appears to be normal," is worthy of note in connection with the considerable pleuritic effusion and collapse of the right lung, both of which undoubtedly existed before that time.
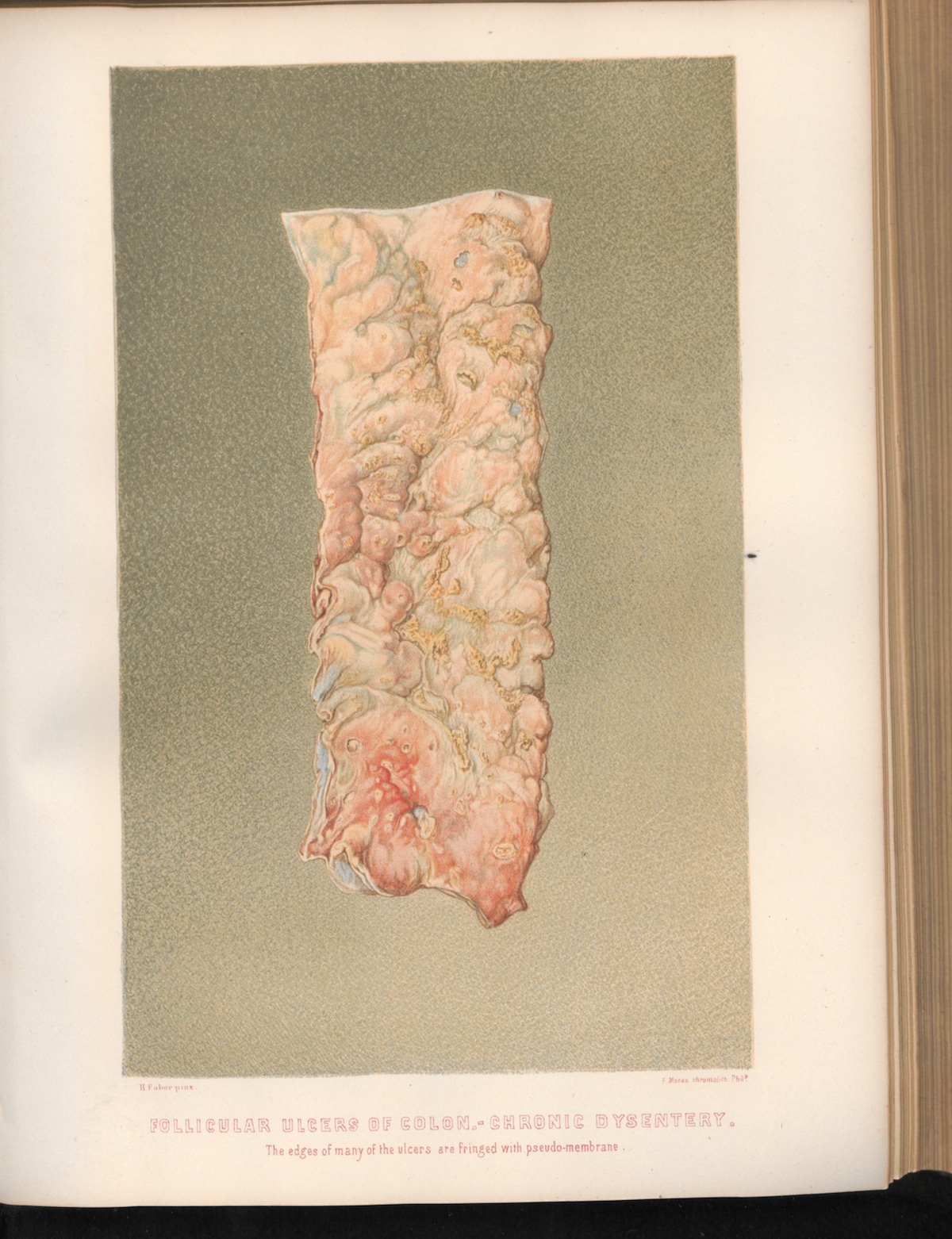 PLATE XXXI. FOLLICULAR ULCERS OF COLON.—CHRONIC
DYSENTERY. The edges of many of the ulcers are fringed with pseudo-membrane.
PLATE XXXI. FOLLICULAR ULCERS OF COLON.—CHRONIC
DYSENTERY. The edges of many of the ulcers are fringed with pseudo-membrane.