Title: Q——, John
Source text: Surgeon General Joseph K. Barnes, United States Army, The Medical and Surgical History of the War of the Rebellion. (1861–65.), Part 1, Volume 2 (Washington, D.C.: Government Printing Office, 1870), 561-562.
Civil War Washington ID: med.d1e20024
TEI/XML: med.d1e20024.xml
CASE 11.—Private John Q——, Co. E, 9th New York Cavalry, sustained a comminuted fracture of the right clavicle, by his horse being shot during a charge into Winchester, Virginia, June 8th, 1862, and falling upon him. He was conveyed to Washington and admitted to Finley Hospital, where he was found to be suffering from general emphysema, the result, probably, of a wound of the apex of the pleura from some of the fragments of the broken bone. He was treated for this difficulty for a considerable time and finally entirely recovered. Several spiculæ of bone were removed through an incision from under the skin in the situation of the sternal extremity of the clavicle. On October 21st, 1863, he was admitted to St. Joseph's Hospital, Central Park, New York. The wound over the sternal aspect was still open and presented the pouting and indolent appearance indicative of dead bone at its bottom. A probe being passed into this opening disclosed bare bone, which was still firm in its attachments and which was decided to be a portion of the head of the clavicle. His condition was good and it was thought best to wait until the sequestrum should detach itself before any attempt at removal should be made. January 14th, 1864, an abscess formed over the outer third of the clavicle which was opened and showed the existence of dead bone at that point also. Simple applications were made to both wounds. February 10th: The sternal extremity of the clavicle commenced to protrude itself through the inner opening and was found to be connected with and evidently to form a solid piece with that portion of sequestrum felt through the outer opening. It was thought that the whole of that portion of the bone between these two points was dead. There was a considerable amount of thickening around it caused by the deposit of involucrum. The wound discharged slightly. June 1st: The bone was now freely movable in its bed and its sternal end pointed out of the wound for a distance of three-fourths of an inch. Aside from a pain in the right side of the chest and in the right shoulder, with an inconvenience in the motion of the parts, the patient suffered very little and enjoyed a good appetite. On June 21st, 1864, Acting Assistant Surgeon J. K. Merritt removed the sequestrum by slightly enlarging the internal opening. The parts from which this portion of bone was removed soon became firmly braced by a new bridge of osseous tissue, formed by the involucrum, and really constituted a new clavicle. The motions of the arm, though somewhat restrained, were nevertheless good, all the support to the shoulder necessary for the subsequent good use of the limb being left good. The case progressed well until July 16th, when the wounds covered themselves with an ashy slough and hospital gangrene fairly declared itself. On the 10th, a thick, angry-looking slough covered both wounds; the edges of the openings were tumid and inflamed. The surfaces of the ulcers were touched with bromine, but the sloughs were so thick that the remedy failed to have the desired effect. On the 14th, the sloughs were removed and bromine applied directly to the part. By the 16th, the gangrene had extended itself into the track which communicated between the two wounds. The patient complained of a great deal of pain and soreness. Bromine was introduced into the track of the wound, but owing to the presence of the slough and the difficulty of removing it, the remedy could not be brought in direct contact with the surfaces underneath. The parts were repeatedly touched with bromine and bathed with a wash made of the same. Under this treatment they assumed a healthy aspect and the patient commenced to do well. By September 19th, the parts had entirely healed; there was a marked enlargement from deposit of new bone at the seat of exfoliation. The soldier was discharged from service October 1st, 1864; the arm was useful and nearly all the normal movements could be made with it. The sequestrum is represented in the adjoining wood-cut (FIG. 258). It is partially tubular and is about three inches in length. The sternal articular surface is destroyed as well as all the cancellous structure in the longitudinal diameter of the bone. It is evident, too, that the acromial end of the clavicle did not become necrosed, and the deficiencies of the compact tissue of the head portion of the bone may be accounted for by the removal of the several small fragments at the hospital at Washington. The excavation on the anterior face of the bone was probably caused by the removal of two or three detached fragments at that time. If there were any small fragments toward the sternal end, as doubtless there were, they must have been firmly attached to the periosteum and become incorporated with the involucrum, and helped to form the firm bridge of bone which exists over the subclavian vessels. The specimen was contributed, with a history of the case, by Acting Assistant Surgeon G. F. Shrady.
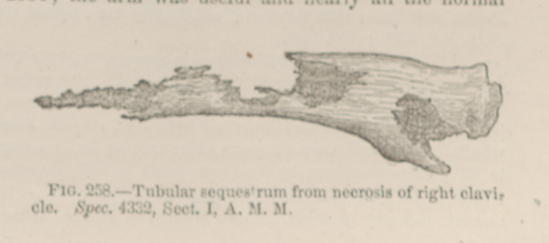 FIG. 258.—Tubular sequestrum from necrosis of right
clavicle. Spec. 4332, Sect. I, A. M. M.
FIG. 258.—Tubular sequestrum from necrosis of right
clavicle. Spec. 4332, Sect. I, A. M. M.