Title: Hughes, Patrick
Source text: Surgeon General Joseph K. Barnes, United States Army, The Medical and Surgical History of the War of the Rebellion. (1861–65.), Part 1, Volume 2 (Washington, D.C.: Government Printing Office, 1870), 206-207.
Civil War Washington ID: med.d1e14556
TEI/XML: med.d1e14556.xml
CASE.—Private Patrick Hughes, Co. K, 4th New York Volunteers, aged 23 years, was wounded at the battle of Antietam, September 17th, 1862, in Sumner's attack on the right, near Dunker's Chapel. Several special reports, at variance in regard to some particulars of the case, have been received. In the note book of Surgeon J. H. Brinton, U. S. V., it is stated that "two missiles had struck the back portion of his head, the one near vertex causing injury of greatest extent," and that "he did not entirely lose his consciousness at time of injury." But the field report, and the majority of the subsequent hospital reports, state very positively that the injury was a perforation of the skull by a single conoidal musket ball entering near the inner posterior angle of the right parietal, and emerging at a higher point of the left parietal, making, after traversing a portion of the brain, a large exit wound. Little is known of the early history of the case, except that the patient dragged himself from the field, and, after a preliminary dressing from Surgeon G. W. Lovejoy of his regiment, was conveyed to a field hospital in a barn near Keedysville, where he remained until the 20th, when he was sent to Hagerstown. The regimental surgeon reports that the shock and depression from the injury was great, but that the patient was conscious and answered questions rationally. There is no report from the Hagerstown hospital, except that the patient was sent to Washington on the 24th. On the 25th, he was received at the Mount Pleasant Hospital. The following is an extract from the report of Acting Assistant Surgeon Thomas Carroll, who had immediate charge of the case, after the patient's admission to Mount Pleasant Hospital: "The ball entered half an inch posterior to the junction of the coronal and sagittal sutures on the median line, passed backward under the scalp and escaped one inch above the occipital protuberance, inflicting a wound four inches in length, producing a compound comminuted fracture of the skull of the same extent. At the time of his admission to the hospital, eight days after the reception of the wound, so much tumefaction of the parts existed that it could not be ascertained whether or not the brain or its membranes were injured. The general condition of the patient was good; suppuration had commenced; no febrile action existed, the pulse was regular, sleep not materially disturbed, mind clear and manifesting no signs of compression of the brain, or inflammation of its membranes. Little, if any, change was perceptible for several days, when the swelling of the scalp and tissues subsided, leaving a prominence nearly, if not altogether, one inch in height, and two and a half or three inches in length of brain substance, in which the pulsation of the arteries could be distinctly observed. From the closest examination that could now be made, it was supposed that the membranes of the brain were not lacerated, though this supposition was by no means certain, as there was reason to believe the brain itself had been penetrated. The chief, and in fact, the only unpleasant symptom complained of by the patient, was an occasional paroxysm of giddiness that occurred at intervals of from ten to fifteen days; the paroxysms continued to return, though less frequently, while he remained in the hospital. Early in December, he was able to sit up and walk about the ward, and was never afterwards much confined to bed. The protuberance now began to subside, and was soon reduced nearly to a level with the skull; numerous pieces of bone were removed as they became detached from the tissues, leaving a complete channel in the cranium from the point where the ball entered to where it emerged. At the time this man was discharged from the service, January 26th, 1863, the wound was nearly healed. There was but little discharge of pus, and with the exception of an occasional recurrence of the paroxysms of giddiness, he suffered but slight inconvenience. The treatment consisted simply in cutting the hair short, and applying cold water dressing locally, paying strict attention to the diet, and administering a cathartic as often as symptoms seemed to indicate its use." Assistant Surgeon C. A. McCall, U. S. A., in charge of Mount Pleasant Hospital, furnished a report of the case, from which the following extracts are made. "The ball passed from about one inch above and to the right of occipital protuberance into the cavity of cranium and emerged at a point on the left of the median line, about one and three-fourths inches from the point of entry; probably a conoidal ball. From the posterior margin of the inferior wound to anterior margin of superior was about four inches. At the time of his admission to hospital, eight days after the injury, so much tumefaction and hardened clot existed, that it was deemed inadvisable to make a very strict examination with a view to determine the extent of lesion. The hair was closely shaved, and cold water dressings applied and patient placed in a sitting posture. The general condition of patient was promising, although all the brain functions appeared clouded, the memory impaired, speech desultory or given in fragments, yet being readily aroused and, generally at such times, answering promptly and clearly. In a short time healthy suppuration was established, febrile action decreased, the pulse became regular, sleep became natural, the mind began to show clearness, and he seemed to lose all symptoms of compression or of inflammation of the brain or its membranes. The swelling and induration of the parts gradually disappeared, leaving in their place a fungus cerebri of considerable size, perhaps an inch in height by two and a half or three inches in length, in which the pulsation could be distinctly seen and felt. The only unpleasant symptom now existing was the occurrence of a paroxysm of giddiness at intervals of ten or twelve days, which symptom continued, although at much greater intervals, during the remainder of his stay at the hospital. The size and extent of the fungus deterred me from using the knife, and I had resort to compression as recommended by the surgeons of France, but with such serious results that I was startled for the safety of my patient, and therefore threw aside all dressing save the simple cerate on soft lint, and proper guard for the delicate tissues. Early in December, he was able to sit up and walk about the wards, and was never afterwards confined to the bed. From this time the fungus commenced to decrease in size, and continued to do so until shortly before his discharge from the service, January 26th, 1863, when it had shrunk below the level of the skull, and both openings had been well covered by cicatricial tissue. During the progress of the case numerous spiculæ of bone were removed as they became detached. The constitutional treatment consisted in paying strict attention to the diet, and exhibiting saline cathartics and turpentine injections as the symptoms seemed to call for. When the soldier left my hands he complained of no inconvenience whatever with the exception of the occasional attack of giddiness, and the fact that he could not see a small object when placed in a position directly on a level and on a middle line between the eyes. Both which defects, I consider, will diminish with time until lost. Shortly before the patient's discharge from Mount Pleasant, an excellent picture of the aspect of the injury at that time was made in water color, under the direction of Surgeon J. H. Brinton, U. S. V., who was then in charge of the Division of Surgical Records of the Surgeon General's Office, and had secured the services of an artist, Mr. Stauch, whose admirable drawing and coloring have furnished some of the best illustrations of this book. The figure on the right of the chromo-lithograph opposite is a good copy of Mr. Stauch's water-color drawing. I take the following memorandum of the case from one of the memorandum books turned over to me by Dr. Brinton: "Gunshot wound of head: The picture of this case was taken at the Surgeon General's Office, whither the man came as an orderly, or on an errand. He was perfectly well. A small carnified cerebral hernia existed at the exit wound, which was healing rapidly. The ball went into cavity of the skull and emerged. No symptoms existed at all, when the patient's portrait was taken. The wound was then some three or four months old. The history of this case, which I took at the time, has been unfortunately mislaid." After this we have the history of the case taken up by the pension examining surgeons. The patient went to Newcastle, Delaware, and was pensioned at four dollars a month, until June, 1869, when his pension was increased to eight dollars a month. Dr. D. W. Maull reports, at this date, that there was a loss of substance of the skull two inches wide and three inches long, leaving a large depression, covered only by the integuments of the cranium. "Through this can be seen at all times the pulsations of the brain. About the cavity the bone is ridged by the union of the fractured margins. There is almost constant dull pain, some loss of hearing, and the sight of the right eye is impaired." Dr. Maull regarded the disability as total. Yet the man worked afterwards in an iron foundry as puddler. On December 20th, 1870, this patient was examined by Doctors William Thomson and W. W. Keen of Philadelphia, who have published an interesting account¹ of his condition at that time, with a photograph, of which a reduced copy is given in the annexed wood-cut, (FIG. 106.) I make the following quotations from this paper: "His memory is quite good, but by no means so good as before the injury. He is rather easily bothered and confused, and more irritable than formerly. The sight of his right eye, he thinks, is poor. Whisky affects him as usual. Sexual power undiminished. He has no paralysis. The wound of entrance * * is marked by a slight depression in the bone, the wound of exit by a hollow two and a half by two inches, and one inch deep. No bone has closed this opening, but the scalp and hair dip down into the hollow. The arterial pulsations are barely perceptible. When recumbent the hollow is gradually obliterated and replaced, in about one minute, by a rounded protuberance. To prevent pain during this change, he supports the parts with his hand. When he coughs, even with moderate force, the depressed scalp instantly hedges up in a cone, which nearly reaches the general level of the skull and obliterates the depression, and then as suddenly subsides." Drs. Keen and Thomson observe that "the complete recovery from paralysis, (as evinced by his subsequent severe labor,) and the almost entire restoration of his mental faculties, are remarkable, especially in view of the probable deep lesion of the brain, both by the primary injury and the subsequent fungus cerebri." They comment also upon "the rapid changes in the state of the cranial contents, due to any change of position, to coughing, etc., as evinced by the effacement of the depression at the wound of exit." The authors also regard the case as of value in throwing light upon the probable anatomy of the optic commissure. Their discussion on this point is given in a foot-note.²
¹ Photographic Review of Medicine and Surgery. Vol. 1, No. 3, p. 26. Philadelphia, February, 1871. J. B. Lippincott & Co.
² "Wollaston, (Phil. Trans. 1824. p. 222,) reasoning from two attacks of transient hemiopsia, occurring in himself, and other cases in friends, appears to have been the first to point out the semi-decussation of the optic nerves at the chiasm. Longet (Traité de Phys., 2d ed. ii, 476) seems to assent to the explanation, though he refers to cases of perfect sight in which it is asserted no chiasm existed; and in his Traité d'Anat. et de Phys. du Syst. Nerv., p. 666, he gives cases of perfect sight in both eyes, in spite of unilateral cerebral atrophy or traumatic lesion. Von Graefe (Archiv, ii, 286) assents cordially to Wollaston's view, admitting that he proposes nothing new, but that which is far too little known. Hubert Airy, (On a Distinct Form of Transient Hemiopsia, Proc. Roy. Soc., Feb. 17th, 1870, in "Nature," i, 444.) after a careful examination of preceding writers, also supports it; and the experiments of Laborde and Leven, (Med. Gaz., Nov. 5th, 1870; from Gaz. Méd. de Paris,) who found atrophy of the right optic nerve following the removal of the superficial right cerebral convolutions, and without any apparent irritative processes, would also point in the same direction. In our own case, the point to which we desire to call special attention is the rigid optical examination of the region between the porus opticus and the macula lutea. The semi-decussation of the nerves at the chiasm being admitted, it would naturally be supposed that the fibres a from the left tract would supply the left retina from the porus opticus toward a'; but our examination shows that it supplies less than this, viz.: only that part of the retina from c to a'; while in the right eye the fibres b, instead of supplying the retina from the porus opticus to b', supply more than this, viz.: that part of the retina from c' to b' . In other words the fibres a and b of the left optic tract supply, mathematically, the left halves of the two retinæ from c to a' and c' to b' , and the right tract the right halves. As to the cerebral seat of the sense of vision, the amount and depth of the injury to the brain are too uncertain, perhaps, to warrant us in venturing on any speculations us to its locality."
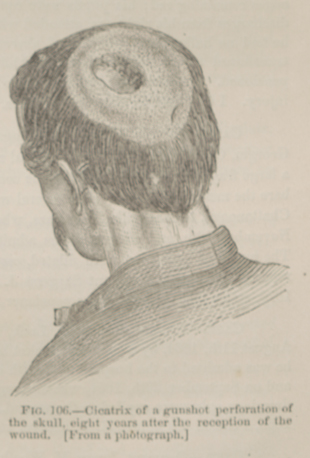 FIG. 106.—Cicatrix of a gunshot perforation of the
skull, eight years after the reception of the wound. [From a photograph.]
FIG. 106.—Cicatrix of a gunshot perforation of the
skull, eight years after the reception of the wound. [From a photograph.]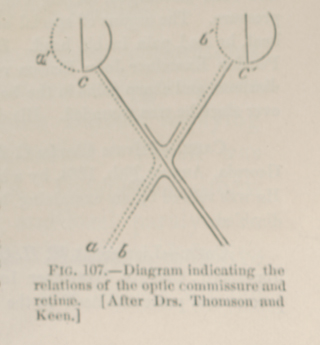 FIG. 107.—Diagram indicating the relations of the
optic commisure and retinæ. [After Drs. Thomson and Keen.]
FIG. 107.—Diagram indicating the relations of the
optic commisure and retinæ. [After Drs. Thomson and Keen.]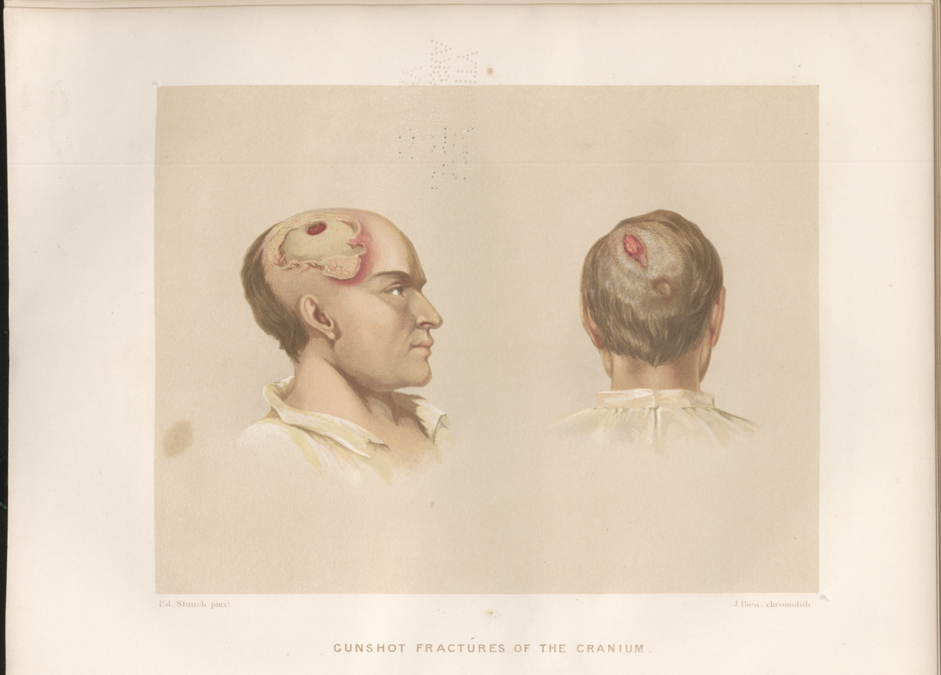 PLATE VI, facing p. 207. GUNSHOT FRACTURES OF THE CRANIUM. Two
figures: Left hand, case of McK——, p. 280; right hand, case of
Hughes, p. 206.
PLATE VI, facing p. 207. GUNSHOT FRACTURES OF THE CRANIUM. Two
figures: Left hand, case of McK——, p. 280; right hand, case of
Hughes, p. 206.