Title: C——, Daniel
Source text: Surgeon General Joseph K. Barnes, United States Army, The Medical and Surgical History of the War of the Rebellion. (1861–65.), Part 1, Volume 2 (Washington, D.C.: Government Printing Office, 1870), 144-145.
Civil War Washington ID: med.d1e10928
TEI/XML: med.d1e10928.xml
CASE 10.—Private Daniel C——, Co. D, 76th New York Volunteers, was wounded at the second battle of Bull Run, August 30th, 1862, by a musket ball which inflicted a long transverse scalp wound near the vertex, the greater portion of the wound being over the right parietal. The wounded man was sent to Washington, and thence to Annapolis, where he was admitted to the General Hospital on September 8th. He was suffering from intermittent fever, and this diagnosis was placed upon his bed card, the wound being regarded as trivial in its nature. Treatment was directed to the interruption of the febrile paroxysms, which recurred obstinately in spite of the free administration of preparations of quinia. On September 23d, Assistant Surgeon J. W. Brewer took charge of the patient. The remainder of this abstract is compiled from his interesting notes of the case. The wound looked well at this date, and gave the patient no uneasiness; it was covered by florid healthy granulations, and discharged, in small quantity, laudable pus. The man had had no chill for twenty-four hours. Quinine was continued in small doses, and a generous diet was ordered. On the following day, September 25th, the patient complained of acute pain over the lower lobe of the right lung. There was no modification of resonance on percussion; and auscultation revealed no alteration in the respiratory murmur. Stupes of turpentine were ordered, and an aperient dose. At noon the pain in the side was much relieved; but the patient complained of violent pain in the right ankle, and in the foot of the same side. The cause of this pain, or of its location, could not be ascertained. At night, the pain was not relieved, and the patient was becoming very restless and irritable, which led Dr. Brewer to suspect some occult cerebral disorder, and again to examine the wound, and, finally, to request Assistant Surgeon T. H. Helsby, U. S. A., to see the patient with him. A careful exploration of the wound failed to detect any injury of the bone, a granulating surface being everywhere presented. In the absence of any symptoms, except restlessness, that could be referred to cerebral disturbance, it was concluded that the wound had no connection with the existing pain and general irritability and the patient was ordered to have an anodyne, and a stimulating embrocation to the ankle. On the following morning, September 25th, 1862, coma suddenly supervened, and death promptly ensued. An autopsy was made, two hours after death, by Acting Assistant Surgeon B. B. Miles. The thoracic viscera were found to be in a normal condition, except that there was inflammatory engorgement, or possibly, hypostatic congestion only, of the lower lobe of the right lung. The abdominal viscera were carefully examined, but no cause of death could be found in that cavity. The calvaria was then removed. The dura mater was adherent to the bone beneath the site of the wound. A depressed stellate fracture of the vitreous table of the right parietal was discovered near the sagittal suture. A small quantity of pus followed the removal of the calvarium. On removing the dura mater, several ounces of pus were found on the surface of the left hemisphere. On closer examination, an aperture was discovered in the falx, and it became evident that an abscess had formed beneath the depressed fracture, and had burst through the falx, inundating the convolutions of the opposite hemisphere. The veins of the lower extremity, and of the lung were not examined, and whether the pain in the right foot and right chest were signs indicative of embolic complications resulting from the abscess was not determined. In concluding his report, Dr. Brewer again calls attention to the fact that no symptoms of encephalitis appeared in the case; but it is to be remembered that the chills, which were reported as paroxysms of intermittent fever, did not come under his observation, and that no record of their attendant symptoms has been preserved. The calvaria was sent to the Army Medical Museum by Dr. Brewer. (FIG. 52 and FIG. 53.) The preparation is described in the Catalogue of the Surgical Section, (p. 8.) It is fairly represented in the foregoing wood-cuts as the vault of the cranium, showing a contusion of the right parietal bone at the middle of its superior border. The outer table is spongy, and a thin plate, one inch in length, is necrosed and partially separated. The internal table is fractured and slightly depressed, and shows traces of an attempt at repair.
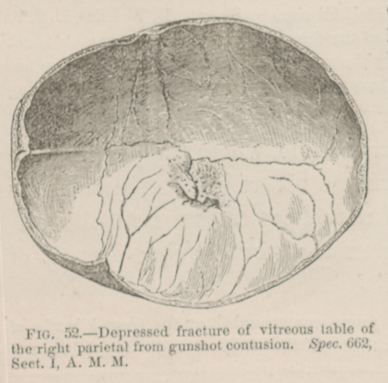 FIG. 52.—Depressed fracture of vitreous table of the
right parietal from gunshot contusion. Spec. 662, Sect. I, A. M.
M.
FIG. 52.—Depressed fracture of vitreous table of the
right parietal from gunshot contusion. Spec. 662, Sect. I, A. M.
M.
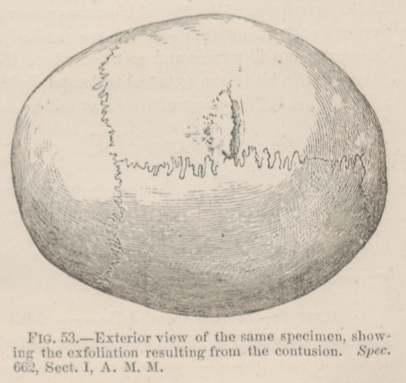 FIG. 53.—Exterior view of the same specimen, showing
the exfoliation resulting from the contusion. Spec. 662, Sect. I,
A. M. M.
FIG. 53.—Exterior view of the same specimen, showing
the exfoliation resulting from the contusion. Spec. 662, Sect. I,
A. M. M.