Title: L——, William
Source text: The Medical and Surgical History of the War of the Rebellion. (1861-65.), Part 2, Volume 2 (Washington, DC: Government Printing Office, 1876), 216.
Civil War Washington ID: med.d2e31891
TEI/XML: med.d2e31891.xml
CASE 630.—Sergeant William L——, Co. D, 10th New York Cavalry, aged 25 years, was admitted to hospital at Alexandria on October 15, 1863, having received a gunshot wound at Bristoe's Station on the previous day. The ball entered the left groin one-half inch to the outside of the femoral artery and half an inch below Poupart's ligament, extending backward; the probe could be passed toward the pelvic cavity for a distance of five inches, but the ball could not be found. At the time of admission there were no symptoms of injury of the abdominal viscera; his general health was good, and there was no derangement of the functions. On October 16th, he was attacked with a violent diarrhœa and had passages of a light-green color; the pain in the groin was slightly relieved and the diarrhœa was partly controlled on the next day, and, on the 19th, he had a slight chill, and there was a yellow discoloration of the skin around the wound; pulse 100, and feeble; patient weak; diarrhœa more severe. The yellow discoloration of the skin increased, and, by the 21st, was decided and general over the whole body and whites of the eyes. On the 22d, the bowels were regular as to the number of passages, but of a loose character and light-green color; pulse 100, and feeble; he had a severe chill, and died five minutes afterward, death being caused by pyæmia. The post-mortem examination showed that the ball had struck the os innominatum and caused a compound impacted fracture of a portion of the bone, two inches square, above the acetabulum. The ball had passed into the pelvic cavity, and was found lying directly under the bladder. The whole course of the intestinal canal as well as the stomach was found highly congested. An abscess was found in the right lobe of the liver containing two and a half ounces of pus, and the whole organ was softened. All the abdominal viscera were congested. The specimen (FIG. 144) consists of the iliac portion of the left acetabulum and adjacent bone, with a conoidal ball (FIG. 145), which has contused the internal surface of the ilium just below and behind the anterior inferior spinous process, and was contributed, together with the history, by Acting Assistant Surgeon J. Hunt Stillwell.
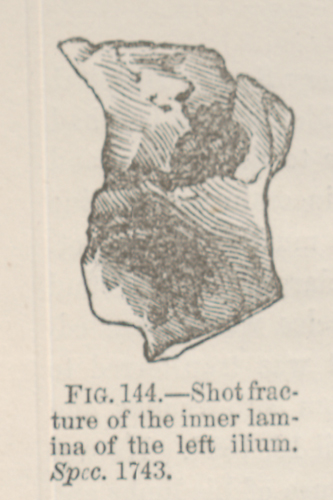 FIG. 144.—Shot fracture of the inner lamina of the left ilium. Spec. 1743.
FIG. 144.—Shot fracture of the inner lamina of the left ilium. Spec. 1743.
 FIG. 145.—Ball taken from the pelvic cavity.
FIG. 145.—Ball taken from the pelvic cavity.