Title: Capps, E. W.
Source text: The Medical and Surgical History of the War of the Rebellion. (1861-65.), Part 3, Volume 2 (Washington, DC: Government Printing Office, 1883), 312-313, 314-315.
Civil War Washington ID: med.d2e14176
TEI/XML: med.d2e14176.xml
CASE 488.—Captain E. W. Capps, Co. C, 15th Virginia Cavalry, aged 35 years, was wounded at Brandy Station, Virginia, October 11, 1863. He was admitted, on October 21st, into Lincoln Hospital, Washington. Assistant Surgeon H. Allen, U. S. A., reported:¹ "A conoidal ball entered the right leg, from without inward, about one and a half inches below the patella, passed through the anterior portion of the leg, fractured the spine of the tibia, and emerged on the inner side of the limb. On admission a bandage was found applied tightly to the affected part. Upon its removal the joint was discovered to be greatly swollen from effusion, and the wounds presented an inflamed appearance. Cold-water dressings were applied. No constitutional symptoms were present. After the effusion in the joint had subsided a thorough examination of the wound was made. The head of the tibia was found pierced by the ball. No stellation existed, nor was the joint involved. A seton of tow was thrust through the wound and withdrawn, bringing away several small fragments of bone. On October 21st, a small abscess was opened in the popliteal space. The patient, from this time, did remarkably well, and all thought him to be out of danger. On January 26, 1864, however, when he was walking, with the assistance of crutches, from one ward to another, he stumbled, and, in order to preserve his balance, bore his weight upon the injured limb. The following day an erysipelatous inflammation set in about the joint, which became enormously swollen. He was restless and uneasy, his skin hot and dry, tongue coated with a thick whitish fur; he had severe pain in the head; pulse 140; anorexia and constipation present. On January 29th, a sense of decided fluctuation was felt in the joint, and it was thought at the time that pyarthrosis of the knee joint was present. He had little or no fever. His pulse averaged 120 beats per minute, soft, compressible. Face very pale, mind clear. The swelling in the course of a week had gone down completely from the limb below and above the joint; but around the seat of injury and joint a dull purplish red color lingered. By judicious pressure pus could readily be made to exude through the internal wound. Pus had burrowed a very little distance in the parts connected with the popliteal abscess above mentioned. No sinus of any extent existed. It was now evident that the case was one demanding amputation, and, the patient's condition being favorable, the circular operation was performed by Assistant Surgeon J. C. McKee, U. S. A., in charge, on February 8th. The joint, which gave evidence of the presence of pus of long standing, the cartilages being denuded and partially destroyed, was sent to the Army Medical Museum (Specimen 2036 of the Surgical Section). The patient did well until February 12th, when he had a severe chill which lasted forty minutes. This was followed by a profuse diaphoresis. The skin became cold and clammy, the pulse 120 and feeble. On the following day he had another chill, and, on the 15th, two more, one in the morning at six, the other at four o'clock in the afternoon. Another exacerbation occurred on the morning of the 16th. In other respects the constitutional symptoms of what was evident to all to be pyæmia were remarkably slight. His tongue remained clean. His appetite continued the same. There was no vomiting, no fever of any consequence followed the chills; his pulse varied from 120 to 140, rapid and weak. His appearance at this time was that of a man who was suffering from a severe hæmorrhage; his anæmic condition was startling; his sclerotica were pearly white, his lips and gums pale, his finger nails blue. He had a slight cough, though no expectoration. His most distressing symptom was the colliquative sweatings, which came on during the night, and which were not apparently connected with the chills. The limb looked well, and there was no unusual amount of pain in it. The flaps were granulating finely. On February 18th the sixth chill took place, and, on the next day, the seventh, followed by vomiting. He now rapidly sank, and died on February 20th, at four o'clock A. M. Autopsy: Rigor mortis marked. Adipose tissue abundant. Limb much swollen and of a tallow color. Upon dissecting out the vessels the tissues of the thigh were found greatly indurated, especially along the course of the Hunterian tract. The interior of the femoral vein was filled with a solid black clot, which was firmly adherent to the walls of the vein. No disintegration noticed. The lower third of the vessel, that which had lain in contact with the suppurating surface of the stump, was stained by a purulent fluid for about two inches from the patulous opening. A curious appearance was observed in one of the small branches of the profunda vein in the upper third of the thigh. It presented the same general aspect seen in the patulous end of the femoral, and was filled with pseudo-pus." A drawing (made by Hospital Steward E. Stauch, and copied in PLATE XXIII, opposite) of the upper two-thirds of the femur, removed at the post-mortem, shows the separation of the periosteum in osteomyelitis. Upon a longitudinal section of the femur (PLATE XLIX, opposite p. 314) the medulla throughout was found to be of a grayish-yellow color, which was more intense at the region of the trochanter than elsewhere. Numerous small abscesses, more or less elliptical, were arranged lineally down the central portion of the medulla. The bone was not thickened or vascular. The periosteum, however, was inflamed, and, at the lower two-thirds of the specimen, was readily stripped from the bone, where it presented the appearance of having been pulled away from the femur by the fibres of the muscles inserted upon it.
¹ A condensed abstract of this case was published by Dr. ALLEN in the American Journal of Medical Sciences, 1865, Vol. XLIX, p. 39, in connection with his Remarks on the Pathological Anatomy of Osteomyelitis, with Cases.
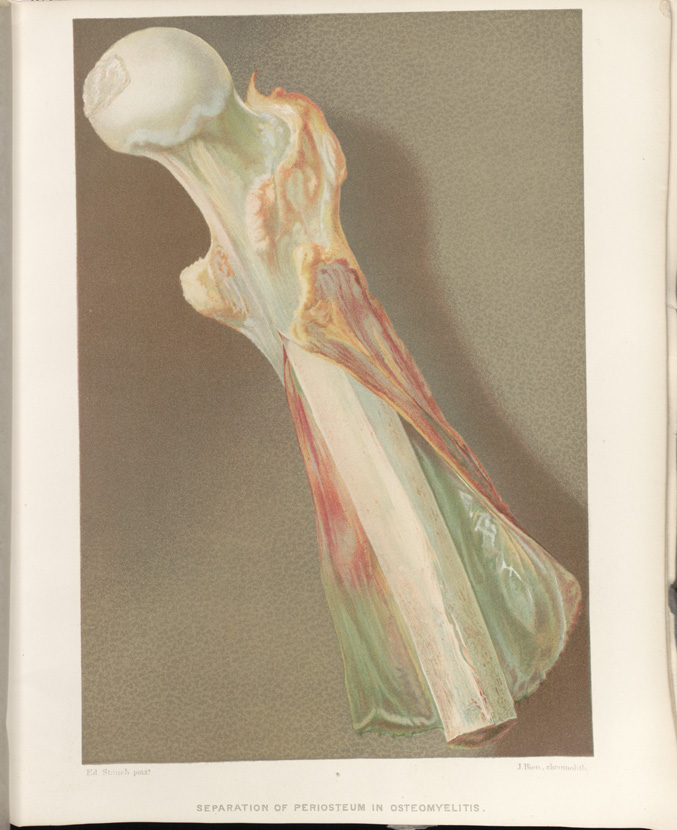 SEPARATION OF PERIOSTRUM IN OSTEOMYELITIS
SEPARATION OF PERIOSTRUM IN OSTEOMYELITIS
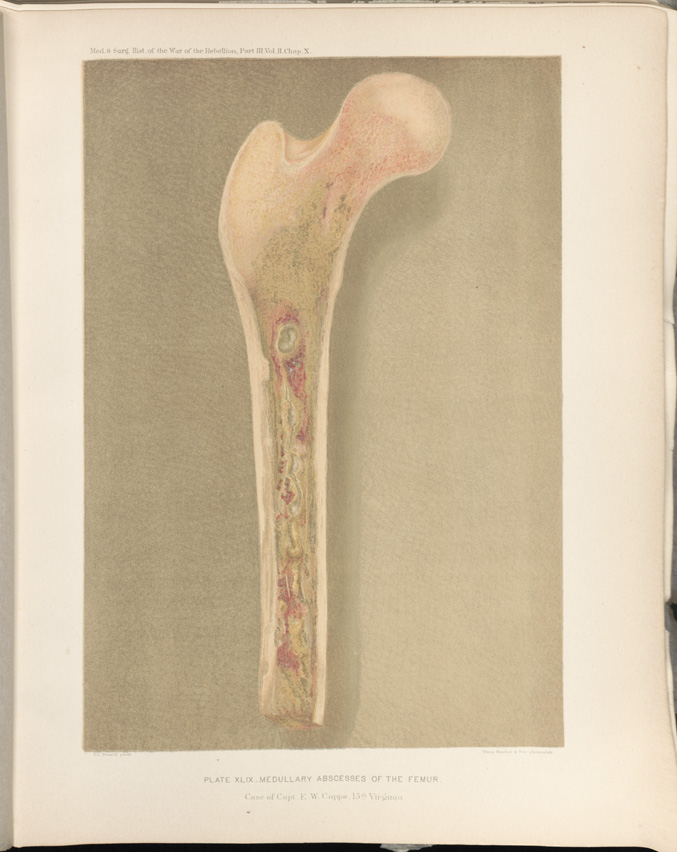 PLATE XLIX __ MEDULLARY ABSCESSES OF THE FEMUR. Case of Captain
E. W. Capps, 15th Virginia
PLATE XLIX __ MEDULLARY ABSCESSES OF THE FEMUR. Case of Captain
E. W. Capps, 15th Virginia