Title: Sailor, W.
Source text: The Medical and Surgical History of the War of the Rebellion. (1861-65.), Part 3, Volume 2 (Washington, DC: Government Printing Office, 1883), 289-290.
Civil War Washington ID: med.d2e12710
TEI/XML: med.d2e12710.xml
CASE 469.—Private W. Sailor, Co. E, 119th Pennsylvania, aged 40 years, was wounded in the left leg by a conical bullet, at Rappahannock Station, November 7, 1863. Two days afterwards he was admitted to Stanton Hospital, Washington, whence Surgeon J. A. Lidell, U. S. V., made the following report: "On examination, it was found that the injured leg was much swollen and dark colored on its anterior surface, that there was no pulsation in the anterior tibial artery, and that both the tibia and fibula were extensively comminuted, with much laceration of the soft parts. His pulse was frequent and irritable, and he had a good deal of constitutional disturbance and fever of an irritative type. On November 14th, the fever had abated, and the general condition much improved; pulse fuller and less irritable; appetite better; wound suppurating; discharge thin, dark colored, and offensive; leg not improved. There being manifestly no hope of saving, it, the bones being broken and the soft parts inflamed nearly up to the knee joint, and comminution very extensive, the limb was amputated in the lower third of the thigh. The operation was performed by the circular method by Assistant Surgeon G. A. Mursick, U. S. V., under sulphuric ether. A dissection of the amputated limb showed that the bones were extensively comminuted as high up as the head of the fibula. The anterior tibial artery was found to be divided by the bullet a little below where it passes through the interosseous membrane, the ends being separated from each other about one inch and retracted within the sheath, also closely contracted. The cardiac end was plugged up by a firm coagulum about an inch in length. The distal end was also plugged up by a small coagulum. The anterior tibial muscles were pale yellow in color, soft and greasy to the touch (fatty degeneration). The patient bore the operation well. The stump was dressed with lead sutures and adhesive plaster, and a full dose of morphine was administered. He had a good night's rest after the operation, and, on the following day, expressed a desire for food, his pulse being full, frequent, and quick; bowels confined, for which a dose of rochelle salts was ordered. On November 17th, suppuration commenced, but little of the stump being united by adhesion; general condition good. Prescribed moderate stimulation, with whiskey. 18th, edge of posterior flap looked sloughy; ordered diluted Labarraque's solution to the stump, and twenty drops of muriated tincture of iron every six hours internally. 20th, had a chill in the morning, followed by fever and sweat; skin sallow looking; granulations in stump looking well, except on the posterior flap, a small portion of which was sloughing. Ordered five grains of quinine every six hours, twenty drops of muriated tincture of iron every four hours, and one ounce of whiskey every three hours. 21st, had a chill in the afternoon; sallow appearance of skin deepened; pulse irritable; slight subsultus; bowels not moved for two days. Ordered ten grains of aloes and twenty grains of rhubarb to be given at once, and continued other treatment. 22d, had chills again in the afternoon, with slight delirium. Ordered one-twelfth of a grain of corrosive sublimate, with three grains of iodide of potassa, every four hours, and continued the whiskey. 23d, patient vomited in the morning, had also a good deal of fever. Applied sinapism to epigastrium. 24th, rigors, etc., in the morning; treatment continued. 25th, rigors, fever, and delirium; skin very yellow. 28th, rigors, etc.; urine passed involuntary; bedsores on sacrum. Ordered a water bed. Patient died, exhausted, on December 1, 1863, the seventeenth day after the amputation and the eleventh day after the advent of the purulent infection. Autopsy twelve hours after death: Rigor mortis well marked; skin yellow; some emaciation; stump swollen and œdematous; femoral artery well plugged up in stump; end of femoral vein well sealed up in stump; femoral vein empty and collapsed from the end up to the valve at the first anastomosing branch, a distance of about six inches; the vein in this situation about as large as the artery; the walls of the vein also much thickened, being about as thick as those of the artery; the lining membrane looking velvety, wrinkled, and dirty gray in color; no pus in vein. From the valve above mentioned up to the mouth of the vena profunda, a distance of about two and a half inches, the femoral vein was filled to distension with fetid broken down liquefied blood, its lining membrane dirty gray colored in this situation, and its walls somewhat thicker than natural; no pus revealed in this locality by the microscope. At the mouth of the vena profunda the femoral vein was plugged up with yellowish whitefibrine; vena profunda and many of its branches filled and knotted with recent coagulum; femoral vein also filled with recent coagulum above the mouth of the profunda to a distance of about two and a half inches; the lining membrane of the profunda and part of the femoral vein last mentioned stained dark red, and the walls of the vessels somewhat thickened in same locality. A thin dark colored recent coagulum, not filling the calibre of the vein, extended the whole length of the external iliac. The end of the femur in the stump (FIG. 2, PLATE XLIII, opposite) was necrosed to the extent of nearly half an inch, and here the periosteum was thickened, varying from a line to one-third of an inch, detached and gangrenous; underlying bone white in color; medullary membrane at end of bone gangrenous and dirty grayish green in color to the depth of about one-third of an inch; medullary membrane elsewhere more vascular than natural, which was well shown by splitting the bone lengthwise with a saw (FIG. 1 of PLATE XLIII, opposite). Three or four small superficial abscesses were formed about the right extremity of the spleen; the rest of that organ was contracted and indurated. Five or six small superficial abscesses were discovered in the lungs, the pulmonary tissue surrounding each of them being consolidated by inflammatory action. The other organs were natural, and the blood did not exhibit any abnormity." The femoral artery (Spec. 1887) and the femoral vein (Spec. 1888), together with three inches of bone from the stump (Spec. 1890), and the section of the spleen containing the metastatic abscesses (Spec. 1889, shown in FIG. 3, PLATE XLIII, opposite), were contributed to the Museum by Dr. Lidell.
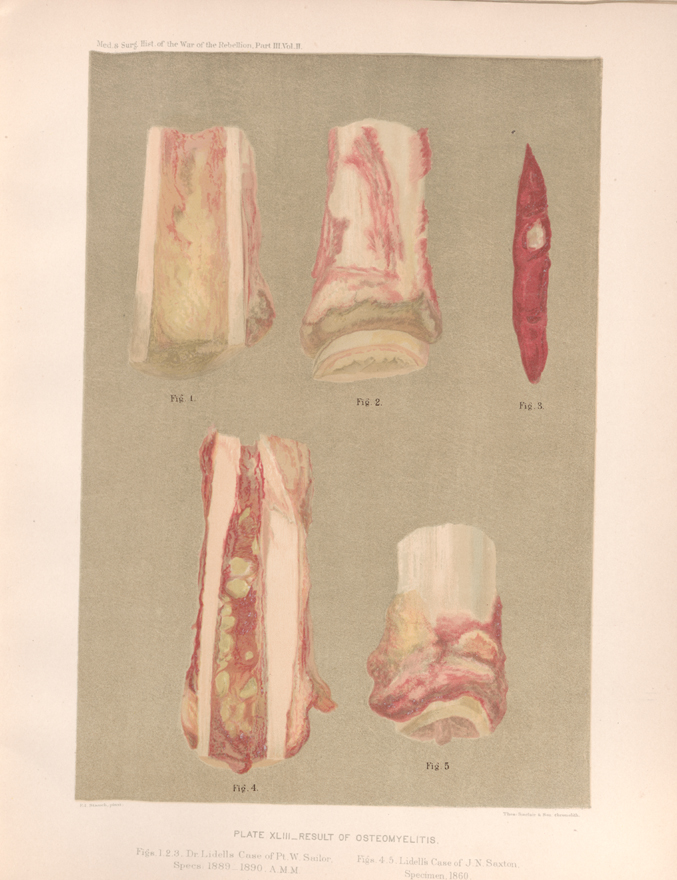 PLATE XLIII. __ RESULT OF OSTEOMYELITIS. Figs. 1, 2, 3. Dr. Lidell's Case of Pt. W. Sailor, Specs. 1889 _ 1890. A. M. M.
PLATE XLIII. __ RESULT OF OSTEOMYELITIS. Figs. 1, 2, 3. Dr. Lidell's Case of Pt. W. Sailor, Specs. 1889 _ 1890. A. M. M.