Title: Vannatta, W.
Source text: The Medical and Surgical History of the War of the Rebellion. (1861-65.), Part 3, Volume 2 (Washington, DC: Government Printing Office, 1883), 242, 287-288.
Civil War Washington ID: med.d2e12175
TEI/XML: med.d2e12175.xml
CASE 464.—Private W. Vannatta, Co. D, 4th Pennsylvania Cavalry, aged 24 years, was wounded at Upperville, June 21, 1863, and entered Stanton Hospital, Washington, three days afterwards. Surgeon J. A. Lidell, U. S. V., reported: "The patient, a man of sound constitution, had received a wound of the right knee by a carbine ball. The missile entered the limb on its anterior inner face a short distance below the joint, passed backward and upward, and escaped through the popliteal space, apparently without opening the joint. From the course and direction of the wound the upper part of the tibia was supposed to be injured. At the time of admission the patient's condition was good, there being no pain, heat, or swelling about the injured knee. He was directed to refrain from using it by remaining quietly in bed, to have ice applied to the wound constantly so as to lessen the danger of inflammatory action, and to be supported by nutritious diet. Under this treatment his case progressed without an untoward symptom until July 5th. At inspection, on this day, I especially noticed his condition as very promising, the anterior orifice of the wound being nearly healed. But, about the middle of the following night, he was seized with great pain and distress in the injured knee, and full doses of morphia were administered without producing much relief. On the following morning the knee was found to be greatly swollen, hot, and exceedingly tender, the patient complaining of intense gnawing pain in it, and crying out from agony occasioned by it. Although his pupils were markedly contracted from the large quantities of anodynes taken, his countenance was expressive of great distress; pulse frequent, quick, and irritable; skin hot and dry: he was also thirsty, had a coated tongue, and had had a slight chill. Free abstraction of blood from the neighborhood of the knee by cups was ordered, also ten grains of calomel, and anodynes as required. On July 7th, the patient's condition had not materially changed. Seeing that the arthritis was secondary to the wound, and believing that it was associated with fracture and comminution of the upper end of the tibia, amputation appeared to be the proper remedy. The operation was accordingly performed by Assistant Surgeon P. C. Davis, U. S. A., in the lower third of the thigh, by the circular method, about midday—thirty-six hours after the attack. Anæsthesia was produced by sulphuric ether. The patient bore the operation well. On examining the amputated limb the inner part of the head of the tibia was found to be extensively injured by the bullet, a deep groove having been made in the bone, associated with much comminution, and some of the broken fragments connected directly with the joint. The cavity of the knee joint was found to contain about four ounces of dirty-brown colored viscid liquid, in which yellowish shining globules (synovia), looking like oil, floated. The lining membrane of the joint was stained with a dull red hue throughout its whole extent and had entirely lost its polished and shining appearance. The internal semilunar cartilage completely covered the opening in the head of the tibia. On July 10th, the patient was progressing pretty well." On October 2d, he was transferred to Turner's Lane Hospital, Philadelphia, where a second operation was performed by Acting Assistant Surgeon C. B. King, who described it as follows: "When admitted, the femur was protruding about half an inch, and appeared to be dead as far up as could be felt with the probe, a ring of new bone being thrown around it. The discharge was very profuse. On October 5th, the patient having been placed under the influence of ether, an oval incision was made around the end of the bone and through the cicatrix and some unhealthy granulations, when, after dissecting the muscles for a short distance, the vitality of the new bone was found to be small, and lateral incisions were made and the flaps dissected up for about four inches, where the new bone seemed to be more healthy, and was sawn off. About four inches of the remaining dead bone, which I judged as reaching up as far as the great trochanter, was extracted with the forceps. The femoral artery was avoided by making the internal lateral incision below the vessel, and the patient lost but little blood. Three or four small arteries were ligated, and the wound was closed with iron wire and adhesive straps. The patient, being very weak from suppuration and the shock of the operation, was rallied with difficulty. Cold-water dressings were applied and stimulants administered. On the following day the patient was still very weak, had a slight fever and coated tongue, and the stump was very much inflamed and swollen. The sutures were removed and the straps loosened, and milk punch, beef tea, and generous diet were ordered. On October 12th, the inflammation was somewhat reduced, the discharge free but very offensive, and the patient was gaining strength slowly and his appetite improving. The ligatures were now removed. On October 18th, the bands were removed, union having taken place in the stump. On November 4th, the wound had closed with an abundance of flap, and the patient was going about on crutches. On November 16th, he was transferred to Haddington Hospital for the purpose of getting an artificial limb." Acting Assistant Surgeon J. R. Levis, in charge of the latter hospital, recorded the following result of the case: "At date of admission a fistulous opening existed in the stump, and on examination by the probe the whole wall of this sinus was found to have an osseous fell leading directly to the end of the femur, where loose spiculae of bone were clearly perceived. A small pledget of sponge tent was applied, and on November, 20th the orifice was well dilated, and, with the dressing forceps, several pieces of bony formation were removed, which crumbled readily under pressure; also a good sized spicula from the sawed surface of the femur. Some inflammation followed this operation, for which lead and opium lotion was applied; perfect quiet was enjoined, and anodynes given at bedtime. On November 23d, the inflammation was still continuing and the patient suffering intense pain in the stump, but two days afterwards both were subsiding. On December 1st, another examination was made by the probe and another small piece of bone was extracted. By December 10th, his health had improved, the discharge had much lessened, and the stump was doing well, the patient stating that it felt better than at any previous time. In January, 1864, the patient went to his home on furlough, and in the following month, when he returned, the discharge had almost ceased. On March 1st, the sinus had closed and the stump was apparently sound." The patient was subsequently transferred to Christian Street Hospital, and was discharged from service June 7, 1864, and pensioned. Examiner J. Walker, of Bethany, Missouri, certified, May 2, 1874: "I find him unable to wear an artificial limb on account of tenderness and shortness of the stump. He is unable to raise the stump in walking, and wears a wooden peg with a leather socket, buckled around his waist. He is also unable to raise the peg, but moves it by moving the side of his body. The stump chafes so easily that he can wear the socket but a short time, and then has to use a crutch." The pensioner was paid June 4, 1879. The bones comprising the knee of the amputated limb were transmitted to the Museum by Surgeon Lidell, and the involucrum and sequestrum, removed at the second operation, together with a cast of the stump, were contributed by the operator. (Cat. Surg. Sect., 1866, pp. 341, 309, and 555, Specs. 1306, 2602, and 1529.) Specimen 2602 is represented in FIG. 1 of PLATE LXX, opposite p. 242.
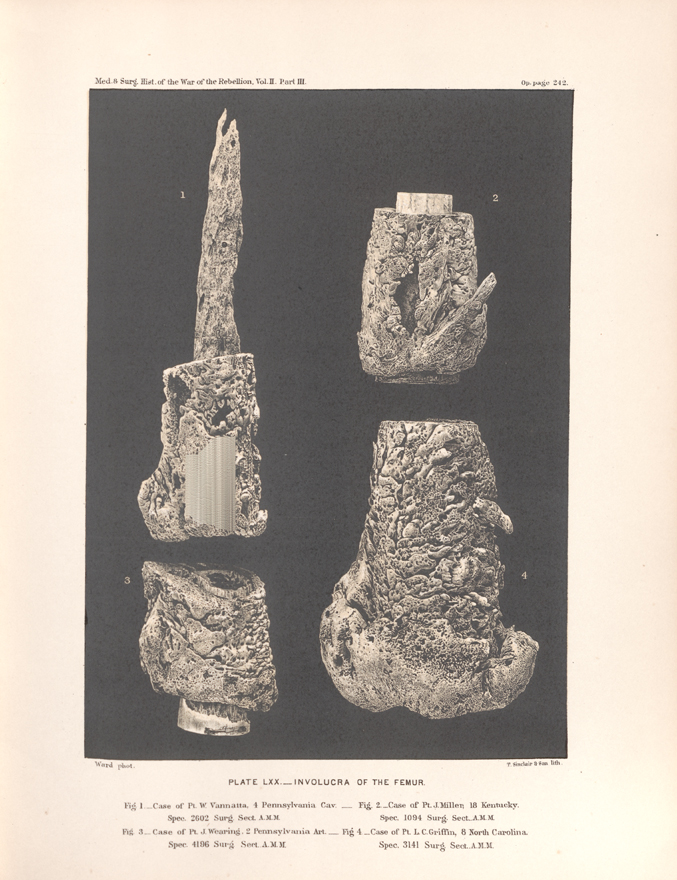 PLATE LXX.__INVOLUCRA OF THE FEMUR. Fig. 1_Case of Pt. W. Vannatta, 4 Pennsylvania Cav., Spec. 2602, Surg. Sect. A. M. M.
PLATE LXX.__INVOLUCRA OF THE FEMUR. Fig. 1_Case of Pt. W. Vannatta, 4 Pennsylvania Cav., Spec. 2602, Surg. Sect. A. M. M.