Title: Jordan, John F.
Source text: Surgeon General Joseph K. Barnes, United States Army, The Medical and Surgical History of the War of the Rebellion. (1861–65.), Part 1, Volume 2 (Washington, D.C.: Government Printing Office, 1870), 543-544.
Civil War Washington ID: med.d1e19872
TEI/XML: med.d1e19872.xml
The complete report is given in the author's own language:²
CASE 20.— "Captain John F. Jordan, Co. B, 13th Virginia Cavalry, aged 31 years, and of sound constitution, was admitted to Stanton United States Army General Hospital, June 23d, 1863. He had been wounded on June 21st, in action near Middleburgh, Virginia, by a shot from a carbine. The bullet, which, by the way, was conical in shape, penetrated the pectoralis major muscle of the left side, at a point on a level with the axillary artery, and about one and a half inches from the margin of the armpit, passed directly backward beneath the shoulder, wounding the axillary artery, together with the brachial plexus of nerves, and escaped behind. Patient said he lost a great deal of blood immediately after the wound was inflicted, so much indeed that he fainted, when the hæmorrhage ceased of itself, and did not return. On admission to hospital, his left arm exhibited some swelling, œdematous in character, and its inner side was ecchymosed nearly down to the elbow-joint. It was also paralyzed, the loss of both sensibilty and mobility being complete. There was no radial pulse in that arm, and pulsation could not be detected in the brachial or any other artery thereof. From this we inferred that the axillary artery had been severed by the bullet. The temperature of the limb was not below the normal standard; on the contrary, we thought it to be somewhat warmer than the limb of the opposite side. There was nothing remarkable in the appearance of the wound. The patient's general condition was good. He did not look as if he had suffered from hæmorrhage. His bowels were constipated; ordered a saline purge, together with a spare diet, and, with a view to lessen the tendency to secondary hæmorrhage, he was directed to remain quiet in bed, to exert himself as little as possible, and to have ice applied constantly over the injured artery. He was also directed to take morphine at night if necessary to procure rest. Under this treatment the patient progressed without an unfavorable symptom; the wound cleaned itself and closed up in a satisfactory manner, and we congratulated the patient in that he was likely to get well without suffering the terrible secondary hæmorrhage, which frequently attends gunshot wounds of the axillary artery. The limb continued to be completely paralyzed as to motion, but sensation had gradually been restored to the fingers, hand, and forearm. On the morning of the 12th of July, we noticed the appearance of a small, rounded, circumscribed swelling of the size of an egg, at the seat of injury to the artery. The scar of the anterior orifice of the gunshot wound was exactly on the summit of the convexity of the swelling, as the patient lay in bed. The tumor was tense in feel, and pulsated distinctly and synchronously with the heart. There was, however, an entire absence of the aneurismal thrill and aneurismal bruit. By compressing the subclavian artery against the first rib, the tumor became soft, much less in size, and ceased to pulsate. On withdrawing compression the tumor speedily filled up, became tense, and pulsated again. Patient stated that during the preceding night he felt something "give way" in his left armpit, while attempting to change the position of this arm by the aid of the right hand. During the day the aneurism increased rapidly in size, and in the evening was fully twice as large as when first noticed in the morning. July 13th, the aneurism continued to increase steadily in size, and in the evening was about half as large as the clenched fist. July 14th, the aneurism had grown but little since previous day; it was still rounded, distinctly circumscribed, and somewhat oval in shape. By compressing the subclavian, it ceased to pulsate, became soft and much shrunken, but the prior condition of things was restored speedily on withdrawing compression; as on a previous occasion, there was still no thrill or bruit. Diagnosis: Circumscribed traumatic aneurism of the axillary artery. From the entire absence of pulsation in all the arteries beyond the aneurism, which existed even at the time of admission to hospital, and the complete want of thrill and bruit in the aneurism itself, we believed that the aneurism had been developed from the proximal end of the severed artery, and that opinion was strengthened by the fact that the swelling had not expanded outward and downward into the armpit, where there was but little in the anatomical structure of the parts to obstruct its growth, any more rapidly than it had done in another direction, where it was covered over and bound down by the pectoral muscles. The swelling had expanded so equally in all directions, that the scar of the anterior wound still remained exactly over the centre of the tumor, as when we first saw it. The aneurism was so distinctly circumscribed that, although its origin was traumatic, it was deemed advisable to attempt a cure of it by the Hunterian method. As there was not sufficient space to secure the artery below the clavicle without opening the sac, I proceeded to tie the left subclavian artery external to the scalenus, on the afternoon of that day (July 14th). The patient being under sulphuric ether, that operation was performed without difficulty by the ordinary method. On tightening the ligature the tumor ceased to pulsate, shrunk a good deal, and became soft. The left arm was directed to be wrapped in cotton wool, and to be kept warm by the further aid of bottles of warm water, to be renewed from time to time as occasion might require. A full dose of morphia was prescribed. He was enjoined to preserve the recumbent posture, and to avoid exertion of every kind. A milk diet was allowed. July 10th, patient had a comfortable night; temperature of arm not diminished: discontinued the warm water. July 16th, patient doing well in every respect; arm warm; color thereof good; discontinued the cotton wool. July 17th, bowels being confined, he took an ounce of sulphate of magnesia. July 19th, aneurismal sac opened spontaneously last night through the anterior sear of the gunshot wound, and discharged two or three ounces of very dark-colored blood, mixed with pus. Suppuration of the sac had been threatened ever since the day after the operation. He was allowed a full diet. July 20th, a moderate discharge of old blood and pus, accompanied with a gradual diminution in the size of the aneurism, and but a moderate degree of inflammation of the sac continued on this and several days following, the patient s general condition being unexceptionable all the while. July 27th, the aneurismal swelling had entirely disappeared; suppuration of the sac, moderate in quantity, still continued, the pus being of a good quality. August 1st, the ligature separated and was removed to-day, without the occurrence of hæmorrhage or any other difficulty; discharge from sac good in quality and steadily diminishing in quantity; discovered some excoriation at the inner side of the left elbow, occasioned probably by pressure, the patient having followed very closely the injunction to keep as still as possible in the recumbent posture; directed a stimulating plaster to be applied, and the pressure to be removed to other situations by arranging pillows. August 5th, discharge from sac had subsided to a small quantity of healthy pus, and the orifice was manifestly contracting. We hoped that adhesion of the sac was taking place. Patient's condition seemed to be favorable in every respect, except that he had been losing flesh rapidly for several days without obvious cause. For want of any other reason, we attributed it to the extreme heat of the weather, the temperature both day and night having been unprecedented ever since July 25th, the mercury at midday ranging from 90° to 100° in the shade, and seldom falling below 80° at night. August 6th: a profuse flow of blood from the sac came on this morning without warning; the loss of blood being so rapid as to threaten speedy death. The officer of the day was close at hand, and stopped the bleeding by injecting about one ounce of liquor ferri persulphatis into the bottom of the sac, through a female catheter, introduced for the purpose. The hæmorrhage ceased immediately. We had been emboldened to use the persulphate of iron freely in this way, because we had a few weeks before (June 22d) stopped a troublesome secondary flow, in alarming quantity, of arterial blood from the cavity of a large abscess, associated with gunshot fracture of the right thigh, by injecting about two drachms of liquor ferri persulphatis through a catheter, carried into the neighborhood of the supposed source of the hæmorrhage, a branch of the profunda artery, and no unpleasant effect of any kind followed it. Again, about the same time, we had been troubled to manage a case of general oozing of blood from the cut surface of a thigh, amputated secondarily for gunshot injury. After trying exposure to the air, ice-water, and even ice, without effect, we stopped this bleeding immediately by covering the end of the stump with pledgets of lint soaked in liquor ferri persulphatis. Aside from pretty severe pain, which soon subsided, no unpleasant consequence of any kind followed. We did not discover any evidence of even the feeblest action as an escharotic, and indeed have since thought that the case progressed better than other amputations of the same class. In consequence of the secondary hæmorrhage and the efforts to repress it, the aneurismal sac became filled up again to the original size. August 10th, another severe hæmorrhage occurred from the same orifice; it was readily stopped by again injecting persulphate of iron in solution. August 11th: profuse hæmorrhage occurred to-day through the opening of the posterior orifice made by the bullet, after it had been healed for more than a month. This bleeding was also suppressed immediately by injecting liquor ferri persulphatis through a catheter. After this there was no more hæmorrhage. During the next few days he seemed to rally from the depression produced by these repeated losses of blood. He was ordered to have wine, and anything in the line of supporting treatment that he would take. August 18th: the aneurismal sac has again suppurated, and there is a profuse discharge of dark-colored and very offensive pus. August 25th: patient failing rapidly; suppuration very profuse and extremely offensive in character. August 29th, he died worn out with the suppuration and the hæmorrhages, forty-six days after the operation, and twenty-eight days after the ligature came away. Autopsy eighteen hours after death: Emaciation extreme; rigor mortis moderate; a large elongated cavity, with ragged dark-colored walls, occupies the original seat of the aneurism, and extends beyond it outward into the axilla; the axillary artery is found to have been severed obliquely by the bullet about one and one-half inches above its termination in the brachial; the divided extremities are separated widely apart (to the extent of about three inches); the distal end appeal s to have been pushed away from the proximal end, either by the original aneurism, or the subsequent hæmorrhages and suppuration; the proximal end is oblique and closed, while the bruised and lacerated portion of it appears about to be cast off by the ulcerative process, as a distinct line of demarcation has been formed; the distal end is oblique and unclosed, but the calibre of the artery is contracted down to about a line in diameter, and it is blocked up by a coagulum three-eighths of an inch long; the branches of the axillary given off above the point of injury, especially the superior thoracic and the acromial thoracic, are much enlarged; the axillary vein is greatly diminished in size about the track of the bullet, but it is still pervious; the brachial plexus of nerves was also wounded by the bullet, all the trunks being cut off except that of the musculo-spiral and circumflex nerves. The proximal extremities of the divided trunks were somewhat bulbous. At the seat of the operation the wound, which at one time was nearly closed, is now open quite down to the artery at the point of ligation, the new granulations having been reabsorbed to that extent, but the artery for a distance on each side thereof is surrounded by a dense mass of new connective tissue, so thick and dense as to make it a little difficult to get at and remove the specimen without injury. On the proximal side of the ligature the vessel is blocked up to a distance of about five-eighths of an inch; on the other side of the ligature it is blocked up to the extent of about two-eighths of an inch. In the cavity of the thorax we find old pleuritic adhesions on both sides, and old tuberculous cicatrices at the apex of each lung; but both lungs are now entirely free from tuberculous deposits; abdomen not opened." The specimen, represented in the above wood-cut (FIG. 249), and also specimen 3243, showing the brachial plexus, were contributed by the operator.
²LIDELL, On the Wounds of Blood-vessels, Traumatic Hæmorrhage, Traumatic Aneurism, and Traumatic Gangrene. In Surgical Memoirs of the War of the Rebellion, Vol. I, p. 101, New York, 1870.
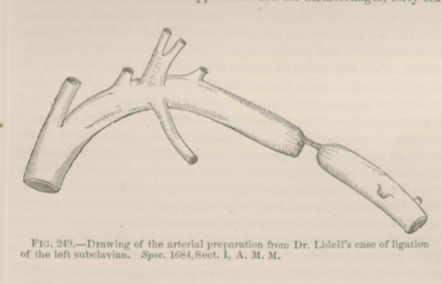 FIG. 249.—Drawing of the arterial preparation from Dr.
Lidell's case of ligation of he left subclavian. Spec. 1684, Sect. I,
A. M. M.
FIG. 249.—Drawing of the arterial preparation from Dr.
Lidell's case of ligation of he left subclavian. Spec. 1684, Sect. I,
A. M. M.