Title: Cotter, W.
Source text: The Medical and Surgical History of the War of the Rebellion. (1861-65.), Part 3, Volume 2 (Washington, DC: Government Printing Office, 1883), 152-153.
Civil War Washington ID: med.d2e6841
TEI/XML: med.d2e6841.xml
CASE 329.—Private W. Cotter, Co. E, 9th New Hampshire, aged 27 years, was wounded at Petersburg, July 30, 1864. Surgeon J. Harris, 7th Rhode Island, recorded his admission to the field hospital of the 2d division, Ninth Corps, and noted: "Fracture of thigh, lower third; amputation of thigh at middle third." From the field hospital the patient was transferred to City Point, and thence to Washington, August 3d. Assistant Surgeon W. F. Norris, U. S. A., contributed the pathological specimen, shown in the wood-cut (FIG. 107), with the following history by Acting Assistant Surgeon H. Gibbons: "The patient was admitted to Douglas Hospital with primary amputation of right thigh, lower part of middle third. The operator had made a long posterior skin flap, which was turned up over the muscles and bone, and attached to the integument anteriorly by means of several sutures. When first seen the stump was greatly swollen, partly from a retention of pus by the bag-like flap. A couple of sutures were removed and the pus evacuated. On August 4th, an incision was made in the dependant portion to admit of free drainage, and poultices were ordered. Appetite and sleep were not greatly disturbed, and there was not as much irritative fever as in most similar cases. Ordered stimulants, tonics, and generous diet. August 13th, swelling much reduced; constitutional irritation less. Ligature of femoral artery separated. The poultices were alternated with flannel dressings till September 1st, when wet cloths were substituted. Flaps mostly united; appetite poor; sleep disturbed; stump painful. Ordered morphia at bed-time. September 13th, patient sits up and walks about with some assistance. Stopped the stimulant. September 28th, stump doing well; swelling gone; dead bone felt with the probe. Had an attack of diarrhœa, which lasted but a few days. The irritability of the stomach was a source of continual complaint for two or three months. The various stomachics relieved but temporarily; nevertheless there was marked improvement, especially during November, the patient being about on his crutches daily. November 29th, divided the cicatrix (but a small fistulous opening was still remaining) and removed a sequestrum nearly six inches long. It was attended with some difficulty, yet not as much as was experienced in similar cases. The sequestrum consists of the entire bone at the lower extremity, but tapers to two or three points at the other; the circumference is complete for three inches. In its centre, surrounding the medulla, was found a beautiful transparent flake of new bone. The femur contained, as in like cases, a large amount of new bone. July 16, 1865, the cavity left in the stump has never entirely closed, but continues to discharge, and refuses to heal, though various stimulating injections have been resorted to. It is over three inches deep. The patient is in a promising state of health." On November 2d, the patient was transferred to the Harewood Hospital. Surgeon R. B. Bontecou, U. S. V., reported that he was doing well on December 31st, but that there was still a "fistulous discharge from the stump." At the closing of the Harewood Hospital, on May 1, 1866, the patient was transferred to the Washington Post Hospital, where the specimen represented in the adjacent cut (FIG. 108) was removed. Assistant Surgeon W. Thomson, U. S. A., who performed the operation, reported as follows: "Two sinuses lead to the interior of new bone, which have failed to close since the date of the first operation. On June 6, 1866, resection of four inches of femur from the end of the stump, after previously made incisions into the soft parts, was performed. Ether was used, and the incisions were united by silver sutures. June 30th, wound has healed kindly, two-thirds by first intention, leaving a sinus on the under surface of the stump still discharging. September 30th, although mostly healed the stump is still indurated. Two sinuses, evidently leading to necrosed fragments of femur, are still open and keep up an offensive discharge. Small intercellular abscesses form occasionally. Patient in good condition." He was discharged from service October 15, 1866, and pensioned. In the following year he was reported as having been treated for a time at the Bellevue Hospital, New York City, where Drs. H. B. Sands and F. H. Hamilton are said to have removed several pieces of necrosed bone. On October 5, 1871, the pensioner entered the Providence Hospital at Washington, with the stump still in a diseased condition; and ten days afterwards Dr. N. S. Lincoln exarticulated the remaining part of the femur, consisting of the head, neck, and trochanteric portions, which was also contributed to the Museum, and is represented in the annexed cut (FIG. 109). The femoral vessels were respected, go that the disarticulation might be said to have resembled an excision or enucleation rather than a reamputation. The patient was able to be about in a short time; and on April 22, 1872, he visited the Army Medical Museum, and a photograph was made of the stump, which is copied in the adjoining wood-cut (FIG. 110). The pensioner subsequently entered the National Military Asylum at Hampton, Elizabeth City County, Va., where Examiner C. McDermont certified the following: "The right leg has been amputated at the hip joint. This was the third amputation performed on the limb. Since the last operation he has been troubled with abscesses in and about the cicatrix, which have not healed, though a year has almost elapsed since the disarticulation was made. It is my belief that the tissues of the wounded limb have been diseased and never free from ulceration since he was wounded. His general health has been considerably impaired by the constant irritation and drain upon his system." This pensioner died at Queenstown, Ireland, January 21, 1874, while on furlough from the Asylum.
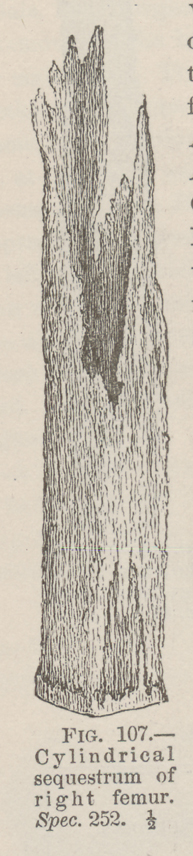 FIG. 107—Cylindrical sequestrum of right femur. Spec. 252. ½
FIG. 107—Cylindrical sequestrum of right femur. Spec. 252. ½
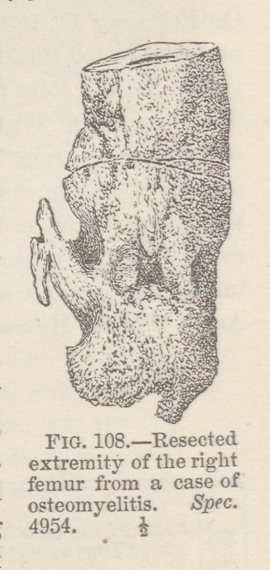 FIG. 108—Resected extremity of the right femur from a case of
osteomyelitis. Spec. 4954. ½
FIG. 108—Resected extremity of the right femur from a case of
osteomyelitis. Spec. 4954. ½
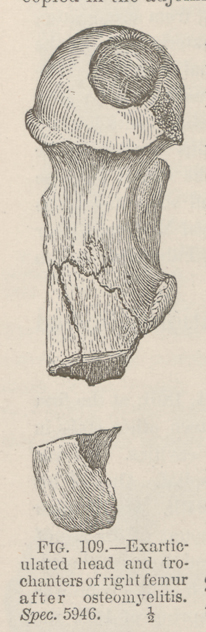 FIG. 109—Exarticulated head and trochanters of right femur
after osteomyelitis. Spec. 5946. ½
FIG. 109—Exarticulated head and trochanters of right femur
after osteomyelitis. Spec. 5946. ½
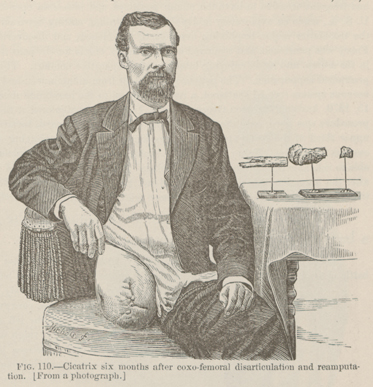 FIG. 110—Cicatrix six months after coxo-femoral
disarticulation and reamputation. [From a photograph.]
FIG. 110—Cicatrix six months after coxo-femoral
disarticulation and reamputation. [From a photograph.]