Title: Wolff, C. M.
Source text: The Medical and Surgical History of the War of the Rebellion. (1861-65.), Part 2, Volume 2 (Washington, DC: Government Printing Office, 1876), 573.
Civil War Washington ID: med.d2e30122
TEI/XML: med.d2e30122.xml
CASE 1554.—Private C. M. Wolff, Co. C, 5th New Hampshire, was wounded at Ream's Station, August 25, 1864, and treated in a Second Corps hospital until the 28th, when he was sent to Lincoln Hospital, at Washington. Acting Assistant Surgeon L. C. Dodge reported: "Wound produced by a minié ball, which entered on the anterior aspect of the left shoulder joint midway between the coracoid and acromion processes, passing directly backward, producing a compound comminuted fracture of the humerus, the ball passing completely through the bone at the surgical neck. The articulating surface of the humerus was not implicated. At the time of admission the arm was considerably swollen as far down as the elbow joint; otherwise, the condition of the patient was good. August 30th: Excision of the upper third of the humerus was performed to-day. A longitudinal incision six inches in length was made, commencing at the acromion process, and passing directly down to the posterior surface of the arm. The fragments of the bone were removed with the forceps, and the shaft of the humerus sawn through; the ordinary dressings were applied." Assistant Surgeon W. Lindsly, U. S. A., noted: "Ether was used as an anæsthetic; six ligatures were used; operation performed by Acting Assistant Surgeon L. C. Dodge." The specimen (FIG. 448), contributed by the operator, consists of the head and one inch and a half of the shaft of the left humerus, excised. A conoidal ball entered the anatomical neck from the rear, fissured the articular surface and shattered the surgical neck, and remains embedded in the specimen. This patient was discharged from service December 3, 1864, and pensioned. E. D. Hudson, M. D., of New York,³ published the following account of this case: "Three months after the operation his arm was healed—some atrophied; not shortened, very flexile, uncontrollable; having an interspace of two and a half inches, which nature had failed to restore; with inability to carry the arm forward across the chest; pectoral and deltoid muscles impaired; nerves, arteries, and functions of the forearm healthy; cannot flex the forearm much for lack of fixedness; carries his forearm in a sling. With apparatus anatomically prepared and applied, scapular pad, and acromion process, a case for the arm attached to the scapular pad, with an oscillatory shoulder joint, and an aponeurotic case for the forearm united to that of the arm with ginglymoid joints; auxiliary straps of rubber webbing for the pectoral and biceps muscles (FIG. 449), he was able to flex the forearm, carry his hand to his head, pronate and supinate the hand, draw it partially across the chest, lift weights with forearm flexed, exercise the forearm, and will regain the use of his arm for ordinary vocations." On December 5, 1864, Examiner Julius Nichols, of Washington, reported: "Removal, by resection, of the head and three and a half inches of the shaft of the humerus; will be partially useful in time; requires perfect rest for one year." Examiner C. O. S. Gilman, of Salem, New York, reported September 25, 1866: * * "he is unable to use the arm for any purpose; it often discharges at the joint; disability total and permanent." This pensioner was paid December 4, 1873.
³ HUDSON (E. D.), Remarks on Exsections, with Cases and Plates, p. 15.
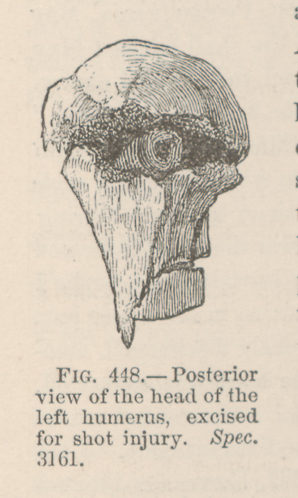 FIG. 448.—Posterior view of the head of the left humerus,
excised for shot injury. Spec. 3161.
FIG. 448.—Posterior view of the head of the left humerus,
excised for shot injury. Spec. 3161.
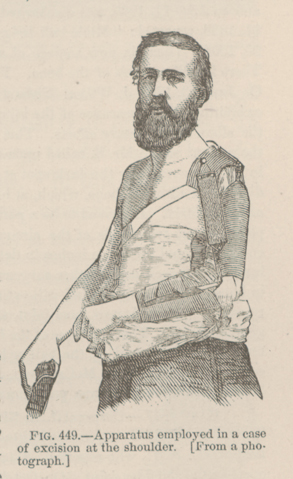 FIG. 449.—Apparatus employed in a case of excision at the
shoulder. [From a photograph.]
FIG. 449.—Apparatus employed in a case of excision at the
shoulder. [From a photograph.]