Title: Coleman, T. P.
Source text: The Medical and Surgical History of the War of the Rebellion. (1861-65.), Part 2, Volume 1 (Washington, DC: Government Printing Office, 1879), 512-513.
Civil War Washington ID: med.d1e41917
TEI/XML: med.d1e41917.xml
There is, however, a curious lesion occasionally encountered in such cases which deserves remark in this place. I allude to the development beneath the mucous membrane of small cysts containing a thick mucoid or glue-like fluid. These vary in size from ⅒th to ¼th of an inch in diameter, and project from the surface in the form of hemispheres; they are sometimes observed in cases of well marked follicular ulceration, but also occur in cases in which no ulceration can be detected. The latter condition was noted in the specimen represented by the chromo plate facing this page. The patient was a confederate prisoner of war, who died of dysenteric diarrhœa of nearly three months duration, which made its appearance while he was under treatment for a gunshot wound of the chest. The following is a brief history of the case:⃰
CASE 899.—Private T. P. Coleman, company A, 19th Mississippi (confederate) volunteers; age 19; was wounded near Petersburg, Virginia, November 5, 1864, by a ball which passed through the lower portion of the left side of his chest, fracturing the eleventh rib and the transverse process of the eleventh dorsal vertebra, and probably wounding the lung. He was treated at first in a confederate hospital at Richmond, Virginia, and, May 6, 1865, was transferred to the hospital at Point Lookout, Maryland. Thence, July 24th, he was transferred to Armory Square hospital, Washington, D. C., and finally, August 17th, to Douglas hospital. The patient stated that on the reception of the injury he had a free hæmorrhage from the wound, spat blood and had great difficulty in breathing, but that he was doing well under treatment, when, about the beginning of June, while still at Point Lookout, diarrhœa set in and persisted in spite of treatment. When he entered Douglas hospital he was still suffering from diarrhœa, which was of a dysenteric character, and he was terribly emaciated. August 18th, the ball, which had lodged behind the tenth rib, about an inch and a half from the wound of entrance, was removed by Asst. Surgeon Wm. F. Norris, U. S. A. His dysenteric diarrhœa was treated by nitrate of silver, used both internally and by injection. He could hardly be prevailed upon to take beef tea or milk, which appeared to make him vomit, but he swallowed whiskey greedily, and it was freely administered. He was restless and noisy, but did not complain of dyspnœa, and had no cough. He sank rapidly, and died August 19th. Autopsy thirteen hours after death: The right pleural sac contained three ounces of sanguineous effusion, and there were old pleuritic adhesions on both sides. The lungs were crepitant, with the exception of the lower lobe of the left lung, which was converted into an abscess cavity containing detritus of lung substance, and the external walls of which were inseparably adherent to the costal pleura. The liver and kidneys were fatty; the spleen contained less blood than usual. The small intestine was pale; in the descending colon and the rectum the solitary follicles were enlarged, forming cyst-like vesicles the size of peas, with minute circular openings at their summits, and each containing a transparent gelatinous mass. History by Acting Assistant Surgeon Carlos Carvallo. [Specimens, viz: No. 660, Medical Section, and No. 1561, Surgical Section, (the injured ribs,) presented by Assistant Surgeon Wm. F. Norris, U. S. A.]
The diseased intestine was brought to the Museum immediately after the autopsy, and a water-color drawing, representing a portion of descending colon, was made by Mr. Hermann Faber; the chromo plate is a reproduction of this drawing. The colon was moderately thickened; the general surface of its mucous membrane was pearl-gray, with greenish and bluish streaks and patches. There were also a number of reddish patches in which congested bloodvessels could be distinctly recognized by the naked eye. The cysts varied in size from ⅒th of an inch or less to ¼th of an inch in diameter; for the most part they were of a bluish color, which in the larger cysts became a dark indigo-blue. At the apices of some of them the yellowish contents shone through, or protruded through tiny circular orifices; these contents could readily be expelled by pressure, and resembled drops of warm boiled glue. The cysts were very unequally scattered over the mucous surface; in some places they were so close as to be in contact; in others they were an inch or more apart. No ulceration was detected anywhere. The minute anatomy of these cysts will be discussed in a subsequent part of this section.
⃰ The history of this case is also given in the first Surgical Volume, p. 568. The account there presented differs from that in the text in stating the diarrhœa to have commenced "about the middle of June," and in speaking of the solitary glands of the colon as "ulcerated." The latter statement is certainly an error, as shown by the specimen, and the former is probably so, as the case-book of the hospital explicitly says "about the beginning of June." Both errors occur in the history, sent to the Museum with the specimens, from which the account in the Surgical Volume was taken, while the history as given above was extracted from the case-book of the hospital, which is the original record.
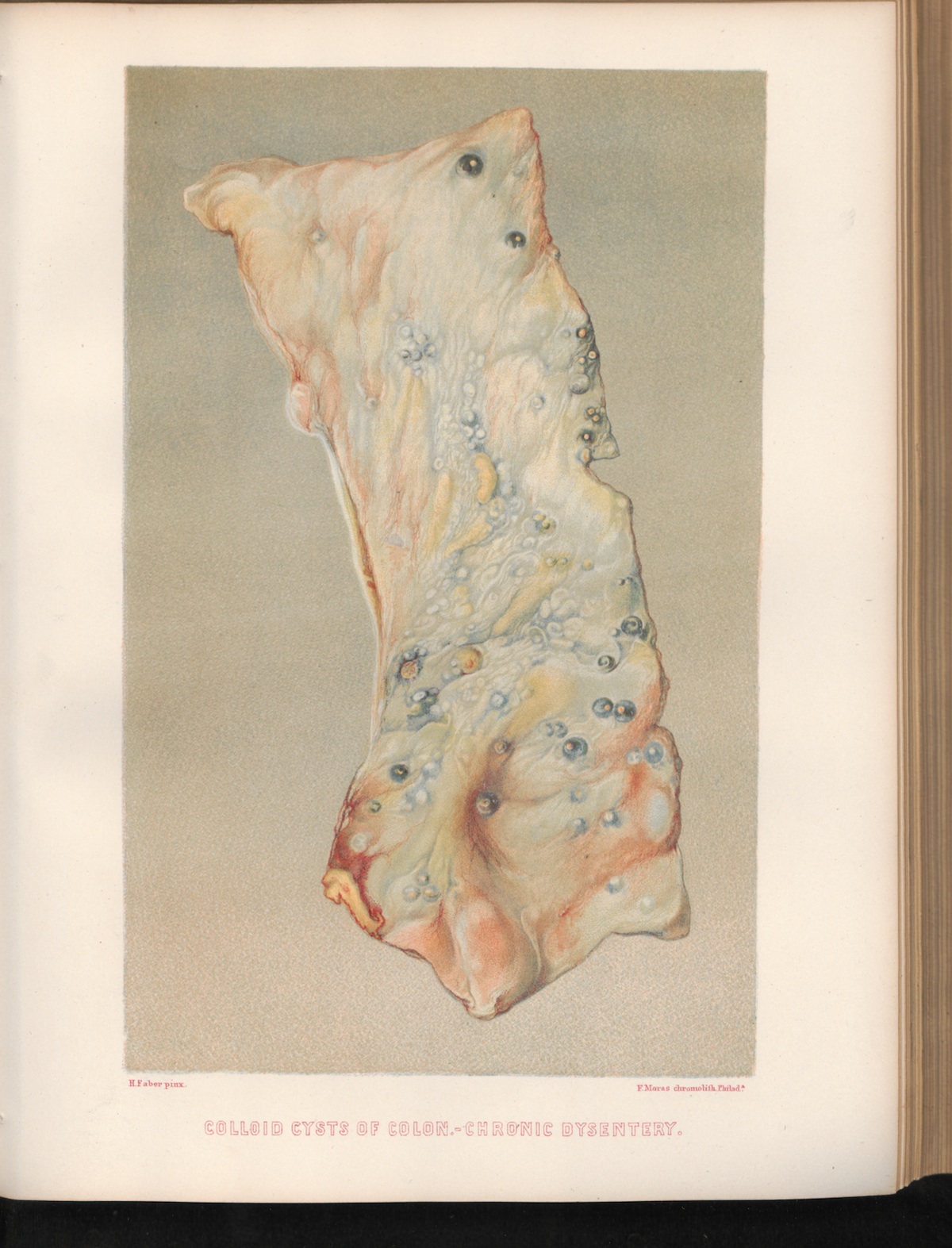 PLATE XXVII. COLLOID CYSTS OF COLON.—CHRONIC
DYSENTERY.
PLATE XXVII. COLLOID CYSTS OF COLON.—CHRONIC
DYSENTERY.